




| Original Article | ||
Open Vet. J.. 2021; 11(4): 747-754 Open Veterinary Journal, (2021), Vol. 11(4): 747–754 Original Research Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castrationInnes K. Wise1*, Heide Klöppel2 and Elizabeth A. Leece31Animal Health Trust, Lanwades Park, Kentford, Suffolk, UK 2Davies Veterinary Specialists, Manor Farm Business Park, Higham Gobion, Hertfordshire, UK 3Paragon Veterinary Referrals, Paragon Business Village, Red Hall Crescent, Wakefield, West Yorkshire, UK *Corresponding Author: Innes Wise. Current address: University of Sydney. Tel.: +61402 061 310. Email: innes.wise [at] sydney.edu.au Submitted: 21/06/2021 Accepted: 01/12/2021 Published: 23/12/2021 © 2021 Open Veterinary Journal
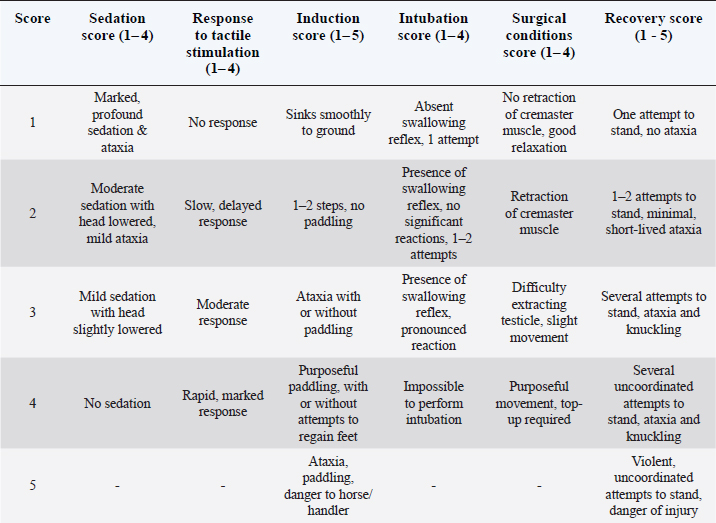
AbstractBackground: Ketamine-based total intravenous anaesthesia techniques are commonly used in equine practice for ponies requiring short procedures such as castration in field conditions. When a longer duration of recumbency than provided by the initial dose of anaesthetic agents is required, administration of supplementary ‘top-up’ doses of anaesthetic agents is required. Ideally, a single dose of anaesthetic agents would reliably achieve a longer duration of action whilst maintaining adequate anaesthetic, surgical and recovery qualities. Aim: This prospective, randomised and blinded study aimed to compare the UK-licensed induction dose of ketamine with an increased dose in ponies undergoing castration in field conditions. The hypothesis was that an increased dose would produce a longer duration of action without negatively affecting qualities of anaesthesia, surgical conditions and recovery. Methods: Ponies were randomly allocated to receive ketamine at either 2.2 mg kg-1 (K2.2) or 3 mg kg-1 (K3) combined with diazepam 20 μg kg-1 following pre-anaesthetic medication with romifidine and butorphanol. Quality of anaesthesia, surgery and recovery were scored using simple descriptive scales (SDS) and timings of key events recorded. Top-up doses of ketamine 0.5 mg kg-1 were administered if anaesthesia was inadequate during surgery. Time of top-up doses and total ketamine doses were recorded. Data were analysed using Student t-tests or the Mann-Whitney U test (p < 0.05). Results: Thirty-six ponies completed the study. Six ponies enrolled were excluded due to cryptorchidism or surgical complications that required deviation from the anaesthetic protocol. There were no differences in timing of events recorded, number of ponies requiring top-up ketamine, timing and frequency of top-ups or total ketamine dose. Scores for anaesthetic and recovery qualities, and surgical conditions were similar between groups. Conclusion: Both induction doses of ketamine provided a similar duration of action and provided conditions suitable to anaesthetise ponies undergoing castration. Keywords: Castration, Equine, Anaesthesia, Ketamine. IntroductionGeneral anaesthesia of ponies using a total intravenous anaesthetic technique (TIVA) under field conditions is commonly required in equine practice. Ideally, the anaesthetic protocol used should be reliable, easily administered, safe for both the animal and attending personnel, and of sufficient duration of action for the surgical procedure. As the anaesthetist is often also the surgeon, administration by a single injection is desirable, avoiding the necessity to administer top-ups of anaesthetic drugs during the surgical procedure. Ketamine is the only induction and maintenance agent licensed for total intravenous anaesthesia (TIVA) of equidae in the United Kingdom (UK). In current UK equine practice, ketamine is commonly administered following premedication with an alpha2 adrenergic agonist and butorphanol (Price et al., 2005; Taylor and Clarke, 2007; Clarke et al., 2014; Lin et al., 2015). Current recommendations in the UK are to administer top-ups of ketamine with an alpha2 agonist every 8 - 10 minutes to maintain a surgical depth of anaesthesia (Zoetis, 2021). Duration of anaesthesia may also be extended by top-up doses of ketamine alone (Kloppel and Leece, 2011; Rigotti et al., 2014; de Vries et al., 2015). Premedication with romifidine, followed by induction of anaesthesia with diazepam and ketamine at the licensed UK dosage of 2.2 mg kg-1 intravenously (IV) provided a duration of anaesthesia of 20.8 ± 2.3 minutes under experimental conditions (Kerr et al., 1996). In this study by Kerr, duration of anaesthesia was defined as the time from induction to when purposeful movement occurred in response to surgical, noise or tactile stimulation. Early pharmacokinetic studies of intravenous ketamine in the horse indicated that increasing the induction dose of ketamine would extend the duration of action (Kaka et al., 1979). This has also been reported in other species (Wright, 1982). Hardðardóttir et al compared 2.2 and 5 mg kg-1 ketamine administered with diazepam 30 μg kg-1 intravenously following premedication with acepromazine 50 μg kg-1, butorphanol 25 μg kg-1 and xylazine 0.7 mg kg-1 in Icelandic ponies undergoing castration in a variety of field conditions (Harethardottir et al., 2019). It was reported that the higher dose rate provided longer duration of a surgical plane of anaesthesia and better surgical conditions for the procedure. However, the higher dose rate caused an increased heart rate and produced an inferior quality of recovery. In contrast, Muir et al reported a similar duration of surgical anaesthesia after administration of ketamine at 6.6 mg kg-1 IV compared to 2.2 mg kg-1 following premedication with xylazine (Muir et al., 1977). This higher dose rate produced poor muscle relaxation during anaesthesia, and recovery was prolonged (93 ± 13 minutes) and of poor quality. Induction of anaesthesia using ketamine at a dose rate of 3 mg kg-1 IV is often used (Benson and Thurmon, 1990) and it is a commonly held clinical impression that this dose provides a longer duration of anaesthesia without adverse effects on anaesthetic qualities of induction, maintenance and recovery. The aim of the current study was to compare the duration of action after administration of ketamine at the licensed dose rate and the increased dose rate of 3 mg kg-1 as part of a commonly used TIVA protocol. The quality of anaesthesia, surgical conditions and recovery were also compared. The hypothesis was that the higher induction dose would provide a longer duration of surgical anaesthesia without negatively affecting anaesthetic and surgical characteristics. Materials and MethodsAnimalsForty-two male Welsh section A ponies, aged 15 months, deemed American Society of Anaesthesiologists (ASA) physical status 1 and scheduled to undergo routine open castration under total intravenous anaesthesia, were enrolled in the study. Ponies were kept in a herd with minimal previous exposure to handling. Each pony was weighed within one week prior to study commencement. On the day of surgery, ponies were group housed in a semi-open barn with straw bedding and free access to water. No abnormalities were detected during pre-anaesthetic physical examination, confirming the ASA grade and hence eligibility. Ponies were randomly assigned to one of two treatment groups undergoing induction of anaesthesia with ketamine at either 2.2 mg kg-1 (group K2.2) or 3 mg kg-1 (group K3). Premedication and anaesthesia inductionPonies were restrained individually in a crush and heart rate (HR), measured by cardiac auscultation, and respiratory rate (fR), measured by observing thoracic excursions, were recorded at rest prior to pre-anaesthetic medication. Each pony was sedated with romifidine (Sedivet, Boehringher Ingelheim, Ellesfield Avenue, Bracknell, Berkshire, RG12 8YS UK) 100 μg kg-1 and butorphanol (Dolorex, Intervet Schering Plough, Walton Manor, Walton, Milton Keynes, Buckinghamshire, MK7 7AJ, UK) 50 μg kg-1 by intravenous injection (IV). Mepivacaine 20 mg (Intra-Epicaine, Dechra Veterinary Products, West Pavilion/Sansaw Business Park, Shrewsbury SY4 4AS, UK) was injected subcutaneously over the left jugular vein before placement of a 14 gauge intravenous catheter (Jelco, Johnson&Johnson International, Leonardo Da Vincilaan 15, 1831 Diegem, Belgium). Following catheter placement, ponies were moved from the crush to a straw-covered area of the barn. Approximately ten minutes following administration of sedation, the level of sedation and the response to tactile stimulation were scored by one of two assessors unaware of treatment group. All scoring systems utilised in the study were simple descriptive scoring systems (SDS) from Klöppel & Leece (Kloppel and Leece, 2011) with a score of 1 representing the best possible score (Table 1). Response to tactile stimulation was assessed by palpating the testicles. If both testicles were not descended normally, the pony was excluded from the study. If sedation was deemed inadequate (a score of 3 or 4) prior to the induction of anaesthesia, romifidine 30 μg kg-1 IV was administered. Immediately prior to induction, HR and fR were recorded. Diazepam (Diazepam Injection, Hameln Pharmaceuticals Ltd, Nexus Gloucester Business Park, Gloucester GL3 4AG, UK) 20 μg kg-1 and ketamine (Narketan 10, Vétoquinol UK Ltd, Pury Hill Business Park, Steadings Barn, Towcester NN12 7LS, UK) at either 2.2 mg kg-1 or 3 mg kg-1 according to group allocation, were combined in the same syringe and administered IV for induction of anaesthesia. The head collar was held for induction, but no other assistance was given. Time from end of induction agent injection to lateral recumbency was recorded. Quality of induction was scored by one of two observers unaware of treatment (Table 1). The ponies were positioned in right lateral recumbency with the left pelvic limb raised to facilitate surgical access. Maintenance of anaesthesia and surgeryOne observer unaware of treatment (IW) performed orotracheal intubation of each pony with a 22 mm silicone uncuffed endotracheal tube and intubation conditions were scored (Table 1). Ponies breathed spontaneously on room air throughout the anaesthetic period. HR and fR were recorded immediately following intubation. Every subsequent five minutes throughout the anaesthetic, recordings were made of HR (by cardiac auscultation), fR (by observing chest excursions), arterial haemoglobin oxygen saturation with the probe placed on the tongue (SpO2; Veterinary Pulse Oximeter PM-60 Vet; Southwest Medical Ltd., 6 & 7, Douglas Road Industrial park, Douglas Rd, Kingswood, Bristol BS15 8PD, UK) and systolic (SAP), diastolic (DAP) and mean (MAP) arterial blood pressures measured oscillometrically with the blood pressure cuff placed around the proximal tail (Cardell® 9401 diagnostic monitor, Sharn Veterinary Inc., 10008 N Dale Mabry Hwy Ste 110, Tampa, FL, USA). Table 1. Simple descriptive scoring systems utilized to score the level of sedation following pre-anaesthetic drug administration, the response to tactile stimulation of both testicles, the quality of induction of anaesthesia, the quality of intubation, the quality of the surgical conditions and the quality of recovery from anaesthesia in 36 ponies. A score of 1 represented the best possible score.
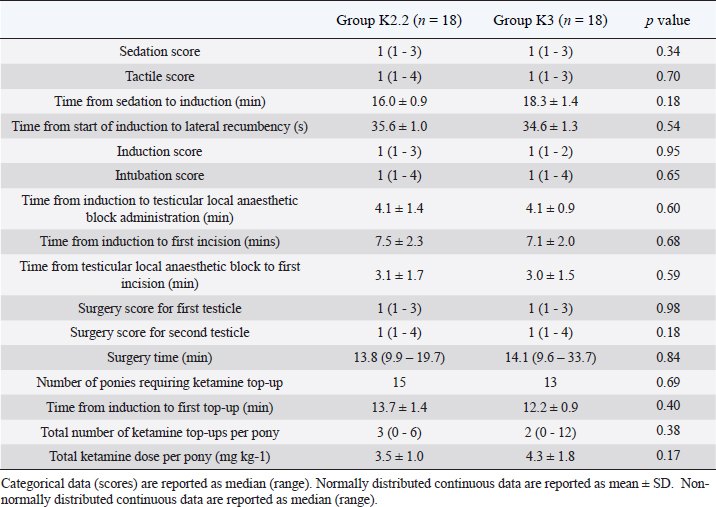
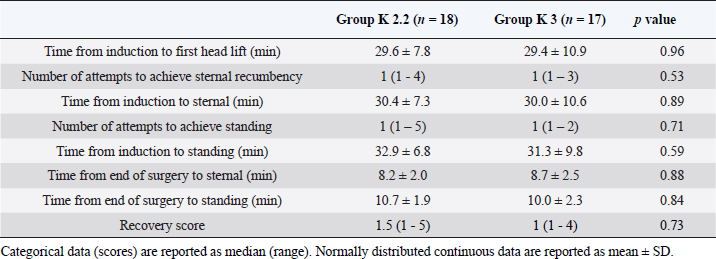
Phenylbutazone (Equipalazone, Dechra Veterinary Products, West Pavilion/Sansaw Business Park, Shrewsbury SY4 4AS, UK) 4.4 mg kg-1 IV, procaine penicillin (Depocillin, Intervet Schering Plough, UK) 12 mg kg-1 intramuscularly and tetanus antitoxin (Tetanus Antitoxin, Intervet Schering Plough, Walton Manor, Walton, Milton Keynes, Buckinghamshire MK7 7AJ, UK) 7500 iu subcutaneously were administered to all ponies prior to surgery. Mepivacaine 1 mg kg-1 was injected intratesticularly prior to surgery. Timings of events under anaesthesia were recorded from the end of injection of induction agent. Times to the start of surgery and to end of surgery were recorded. Castration was performed by one of three surgeons unaware of treatment, using an open technique. Times to exteriorisation of each testicle were recorded and surgical conditions were scored by the surgeon when emasculators were applied (Table 1). If a response to surgery was seen (purposeful movement or swallowing) a top-up dose of ketamine 0.5 mg kg-1 IV was administered by the same observer unaware of treatment (IW) and its use recorded. Anaesthetic duration time was defined as the time from anaesthetic induction agent administration until the end of surgery. Recovery from anaesthesiaThe trachea was extubated at the end of surgery and the ponies were allowed to recover unassisted on deep straw bedding. Recordings were made of times from the end of surgery to first head lift, attainment of sternal recumbency, and standing. Recovery time was defined as from end of surgery until standing. The number of attempts to achieve sternal recumbency and standing were recorded, and the recovery quality scored by one of two observers unaware of treatment (Table 1). Statistical analysisCategorical data (scores) are reported as median (range). Continuous data (weights and times) were assessed for normality using the D’Agostino & Pearson omnibus normality test. Continuous data are reported as mean ± SD if normally distributed and as median (range) if non-normally distributed. Normally distributed data was compared using the Student t tests and non-normally distributed data was compared using Mann-Whitney U tests. Categorical data (e.g. descriptive scores) were evaluated using Mann-Whitney U tests. The level of significance was defined as p < 0.05. Table 2. Simple descriptive scores, defined time points and ketamine doses from sedation to end of surgery in 36 ponies undergoing field castration after pre-anaesthetic medication with intravenous (IV) romifidine 100 μg kg-1 and butorphanol 50 μg kg-1. Anaesthesia was induced with diazepam 20 μg kg-1 IV combined with ketamine at either 2.2 mg kg-1 (Group K2.2, n=18) or 3 mg kg-1 (Group K3, n=18). Ponies received top-up doses of ketamine 0.5 mg kg-1 IV if required to maintain a surgical depth of anaesthesia for the procedure.
Ethical approvalThe study was approved by the Research Ethics Committee of the Animal Health Trust, Newmarket (UK) and performed in 2009 and 2010. ResultsEighteen ponies in each group were included in the study. Study exclusions were three ponies from group K2.2 and two from group K3 due to cryptorchidism. One further pony in group K3 was excluded due to a delay from sedation to induction which necessitated deviation from the anaesthetic protocol. Recovery data of one pony from group K3 was excluded from data analysis due to surgical complications which necessitated deviation from the anaesthetic protocol to maintain more prolonged surgical anaesthesia. There was no difference in body weight between the two groups (K2.2, 173 ± 6 kg; K3, 169 ± 5 kg; p=0.55). Recorded variables and SDS scores for sedation, anaesthesia and surgery are presented in Table 2. One pony in each group required an additional dose of romifidine prior to induction due to insufficient sedation. Both ponies received a score of one for final sedation and tactile scores prior to induction. There were no significant differences in SDS scores in all categories. One pony in each group could not be oro-tracheally intubated following induction of anaesthesia Timings of anaesthetic, surgical and recovery events were not significantly different between groups. The results describing timings of ketamine top-ups, the number of top-ups and the total ketamine doses administered were not significantly different between groups. Recovery timings and scores are presented in Table 3. There was no significant difference in timings of events during recovery or in recovery scores between groups. Table 3. Recovery times (mean ± SD) and scores [median (range)]. See Table 1 for details of animals and drugs.
DiscussionIt is well established that TIVA for horses undergoing short procedures in field conditions using the licensed dose of ketamine for induction following premedication with an alpha2 agonist provides reliable effects and desirable qualities of anaesthesia and recovery (Clarke et al., 2014). However, equine practitioners can require a longer duration of action than provided by the induction dose of anaesthetic agents. Ideally, a longer recumbency time would be achieved without the need for top-up doses of anaesthetic agents, given the typically limited number of trained personnel available in field conditions. This study aimed to determine if a higher induction dose of ketamine than currently licensed could provide an extended duration of action while maintaining acceptable anaesthetic and recovery qualities. This study showed that a dose rate of 3 mg kg-1 ketamine for induction of anaesthesia in ponies did not provide a significantly longer duration of action compared to the licensed dose rate before the requirement for top up doses. However, the characteristics of anaesthesia, surgical conditions and recovery were similar between the two induction doses of ketamine studied. Duration of anaesthesiaMuir et al. (1977) similarly reported a comparable duration of anaesthesia using a single ketamine induction dose at a rate of either 2.2 mg kg-1 or 6.6 mg kg-1 following premedication with xylazine in only three horses under field conditions. In contrast to the present study, the higher dose was evaluated in horses experimentally that were not undergoing a surgical procedure. The horses also received a shorter acting alpha2 agonist alone as premedication. Using longer-acting alpha2 agonists such as detomidine or romifidine have been reported to provide a longer duration of ketamine-based anaesthesia (Kerr et al., 1996; Smith et al., 2020). Both the sedative and analgesic effects of alpha2 agonists potentiate the effects of other anaesthetic and analgesic agents (England and Clarke, 1996). It has been reported that significant sedation is maintained for 60 minutes following administration of a similar dose of romifidine in thoroughbred horses (Wojtasiak-Wypart et al., 2012), and in ponies receiving romifidine with and without butorphanol (Clarke et al., 1991). In comparison, an equipotent dose of xylazine produced significant sedation for 30 minutes following IV administration (England et al., 1996; Clarke et al., 2014). Duration of analgesia provided by alpha2 agonists under experimental and clinical conditions has been reported variably, but often as mirroring the course of sedation (Peboni Figueiredo et al., 2005). Inclusion of a benzodiazepine for induction of anaesthesia has also been demonstrated to extend the duration of action of ketamine-based anaesthesia in ponies following premedication with detomidine under clinical conditions (Allison et al., 2018). Marntell also reported that a romifidine-ketamine-midazolam combination provided an increased time to response to a noxious stimulus compared to a romifidine-ketamine combination administered to horses under experimental conditions (Marntell and Nyman, 1996). Direct comparisons of the current findings regarding duration of action with clinical studies examining higher induction doses of ketamine for induction of anaesthesia in horses or ponies undergoing castration that received top up doses of ketamine as required is difficult due to differences in study design and the data reported. Hardðardóttir et al. (2019) reported on Icelandic ponies undergoing castration in variable field conditions. The ponies were premedicated with acepromazine, butorphanol and xylazine, and anaesthesia was induced with either 2.2 mg kg-1 or 5 mg kg-1 of ketamine with diazepam. The group receiving the higher induction dose received fewer top ups which led the authors to conclude that this provided a longer duration of action. However, data on when the first top up was administered and the total dose of ketamine received was not reported. Rossetti et al. (2008) studied the licensed induction dose of racemic ketamine with 2.5 mg kg-1 s-ketamine, equipotent to approximately 5 mg kg-1 racemic ketamine (Larenza et al., 2008), combined with diazepam in adult stallions undergoing castration and premedicated with romifidine. Top up doses consisted of 25% of the induction dose of ketamine. This study reported that the time to first top up (no later than 7 minutes after induction) was not significantly different between groups. However, the group that received the equivalent higher induction dose received 32% less top up doses compared to the stallions that received the licensed dose of racemic ketamine. The authors interpreted the results as the equivalent higher dose providing a longer duration of action. The most directly comparable reported results with regards to time to first top up when the licensed dose of ketamine was utilized are from Klöppel and Leece (2011) and Rigotti et al. (2014). These studies reported on very similar cohorts of ponies being anaesthetized for castration, under conditions and with an anaesthetic protocol comparable to the current study. In both studies, the time to first top up was approximately 12 minutes for ponies receiving the licensed dose of ketamine for induction of anaesthesia, in agreement with both groups of ponies in the current study. Time to first top up in horses anaesthetized with romifidine, l-methadone, diazepam and s-ketamine at 2.5 mg kg-1 (equivalent to a dose of racemic ketamine higher than the licensed dose) for castration has been reported by Casoni et al as between 10 – 13 minutes (Casoni et al., 2015). This study concluded that the mean duration of surgical anaesthesia when using this protocol was 12 minutes. More recent pharmacokinetic studies using more sensitive assay methods than were available to Kaka et al. (1979) may explain why no significant difference in duration of action was identified between dose rates in both the current study and that of Casoni et al. (2015). In the horse, the rapid redistribution from the central compartment is almost entirely responsible for the often-abrupt offset of anaesthetic action (Waterman et al., 1987; Casoni et al., 2015). This contrasts with other species where hepatic metabolism and excretion contribute to the termination of the anaesthetic effect of ketamine (Casoni et al., 2015). Quality of anaesthesiaIt is widely considered that the induction and recovery periods of anaesthesia present the highest level of danger to both horses and attending personnel. This is particularly true in field conditions – typically a less controlled environment with less equipment and trained personnel available compared to a hospital setting. Good induction qualities were demonstrated in both groups of ponies in the current study. Similar findings were also reported by Hardðardóttir et al. (2019) and Casoni et al. (2015) using higher than licensed doses of ketamine and s-ketamine, respectfully, combined with diazepam when administered to horses in a heavy plane of sedation. The inclusion of midazolam with ketamine for induction improves induction quality by contributing to muscle relaxation (Allison et al., 2018) and comparable effects have been demonstrated using diazepam in a similar manner (Marntell and Nyman, 1996; de Vries et al., 2015), as utilized by Hardðardóttir et al. (2019) Casoni et al. (2015) and in the current study. Heavy sedation prior to induction of anaesthesia with ketamine with has been recommended to produce an acceptable quality of induction (Muir et al., 1977; Matthews et al., 1991). Due to logistical reasons, time from romifidine administration to induction in the current study was longer than the 8 – 10 minutes recommended in the ketamine data sheet (Zoetis, 2021). However, romifidine produces dose-dependent long-acting sedation compared to xylazine and detomidine in both horses and ponies (Clarke et al., 1991; Wojtasiak-Wypart et al., 2012). The pharmacodynamic sedative effects closely resemble the pharmacokinetics. In horses, it has been demonstrated that prominent sedation occurs between 10 – 60 minutes following administration of a similar dose rate of romifidine used in this study. In contrast to the good quality of induction in both groups of ponies in the current study, Rossetti et al. (2008) found adult stallions sedated with romifidine alone, followed by induction with s-ketamine 2.5 mg kg-1 and diazepam demonstrated earlier recumbency, minor excitatory effects and thus an inferior induction quality compared to stallions receiving the licensed dose of racemic ketamine. The administration of butorphanol with romifidine has been demonstrated to augment sedation (Clarke et al., 1991) due to the likely synergistic effects between opioids and alpha2 agonists (England and Clarke, 1996). This may account for the contrasting results of Rossetti, despite the stallions in his study receiving good scores for sedation with romifidine alone. Recovery quality has been widely reported as consistently acceptable following alpha2 agonist/opioid/benzodiazepine-based anaesthetic protocols with the licensed induction dose of ketamine (Kerr et al., 1996; Kloppel and Leece, 2011; Rigotti et al., 2014; de Vries et al., 2015). High-dose ketamine anaesthesia (6.6 mg kg-1) following xylazine administration produced a prolonged recovery period of 93 ± 13 mins that featured increased muscle rigidity, tremors, extreme incoordination, excitement and rotatory nystagmus (Muir et al., 1977). These findings may have historically discouraged equine practitioners from using higher doses of ketamine for induction of anaesthesia. Recovery quality was reported by Hardðardóttir et al as inferior for the horses receiving an induction dose of 5 mg kg-1 ketamine compared to the licensed dose due to a significantly higher number of falls during attempts to stand in the group receiving the higher induction dose (Harethardottir et al., 2019). Both previous studies assessed similar aspects of recovery as the current study. In contrast to these previous studies, both groups in the current study received similar and acceptable recovery scores. A contributing factor to the differing recovery qualities may be that previous studies used the shorter-acting alpha2 agonist xylazine. Sedation and muscle relaxation may have been significantly waning in the recovery period, thus allowing the undesirable behavioural effects of ketamine to become more prominent and thus worsen recovery quality. It has been established that maintaining adequate sedation provided by an alpha2 agonist during the recovery period following injectable anaesthesia improves recovery quality (Muir et al., 1977; Kerr et al., 1996; Marntell et al., 2006). The sedative effect of romifidine would have persisted in recovery in the current study, given the time elapsed between administration of romifidine and the recovery period in both groups (Wojtasiak-Wypart et al., 2012). This may explain the contrast in recovery scores compared to Hardðardóttir et al. (2019). Additionally, the induction doses of ketamine utilized by Hardðardóttir et al. (2019) and Muir et al. (1977) were 60–110% higher, respectfully than in the high-dose group in the present study. Norketamine, the primary metabolite of ketamine, is partially as active as the parent compound and is believed to contribute to adverse prolonged behavioural effects (Clarke, 2014). Bolus administration of 2.2 mg kg-1 ketamine after xylazine sedation in horses has reported to have produced peak plasma levels of norketamine between 8 and 15 minutes after ketamine administration (Waterman et al., 1987). Thereafter, plasma norketamine levels declined very slowly. Therefore, the much higher ketamine induction doses studied by Hardðardóttir et al. (2019) and Muir et al. (1977) may have had the confounding factors of both less sedation from xylazine and higher plasma levels of norketamine compared to the current study that contributed to a poorer recovery quality. Study limitationsThe unvalidated subjective scoring systems used in this study were chosen for their simplicity to use. However, the sensitivity of such scoring systems may not have been great enough to detect subtle but perhaps significant differences in anaesthetic and surgical qualities, as suggested by Kerr et al. (1996). These systems also rely on a degree of interpretation that can vary depending on the individual utilizing them, thus leading to interobserver variability which may have occurred in the current study (Farmer et al., 2014). Utilisation of a visual analogue system or one that considers more aspects of anaesthetic characteristics may have improved the sensitivity of scoring, as described by others (Donaldson et al., 2000; Corletto et al., 2005; Farmer et al., 2014). Another limitation of the current study is the possibility that the study may have been underpowered and therefore limit the degree of interpretation of the data. ConclusionThe results of this study suggest that in ponies, the higher dose of ketamine used preserved acceptable anaesthetic, surgical and recovery qualities as typically observed with the licensed dose. However, the higher dose of ketamine did not provide a significantly longer duration of action as the licensed dose when used as part of a balanced intravenous anaesthesia protocol in ponies. These results suggest that there may be no advantage in using the higher dose studied compared to the licensed dose in ponies. These may be important findings for equine practitioners undertaking anaesthesia in field conditions. AcknowledgmentsThe authors would like to thank Fernando Montesso for his technical assistance in performing this study. Conflict of InterestThe authors declare that there is no conflict of interest. Author ContributionsConceptualization, E.A.L. and I.K.W.; methodology, E.A.L.; software, E.A.L.; formal analysis, E.A.L. and I.K.W.; data curation, I.K.W. and H.K.; writing—original draft preparation, I.K.W.; writing—review and editing, E.A.L and H.K. All authors have read and agreed to the published version of the manuscript. ReferencesAllison, A., Robinson, R., Jolliffe, C. and Taylor, P.M. 2018. Evaluation of the use of midazolam as a co-induction agent with ketamine for anaesthesia in sedated ponies undergoing field castration. Equine Vet. J. 50(3), 321-326. Benson, G.J. and Thurmon, J.C. 1990. Intravenous Anesthesia. Vet. Clin. North Am. Equine Pract. 6(3), 513-528. Casoni, D., Spadavecchia, C., Wampfler, B., Thormann, W. and Levionnois, O.L. 2015. Clinical and pharmacokinetic evaluation of S-ketamine for intravenous general anaesthesia in horses undergoing field castration. Acta Vet. Scand. 57, 21. Clarke, K.W. 2014. Chapter 6 - General pharmacology of the injectable agents used in anaesthesia. Veterinary Anaesthesia (Eleventh Edition), Oxford, W.B. Saunders. Clarke, K.W., England, G.C.W. and Goossens, L. 1991. Sedative and cardiovascular effects of romifidine, alone and in combination with butorphanol, in the horse. J. Vet. Anaesth. 18(1), 25-29. Clarke, K.W., Trim, C.M. and Hall, L.W.A. 2014. Anaesthesia of the Horse. Veterinary Anaesthesia, Saunders Elsevier. Corletto, F., Raisis, A.A. and Brearley, J.C. 2005. Comparison of morphine and butorphanol as pre-anaesthetic agents in combination with romifidine for field castration in ponies. Vet. Anaesth. Analg. 32(1), 16-22. de Vries, A., Thomson, S. and Taylor, P.M. 2015. Comparison of midazolam and diazepam as co-induction agents with ketamine for anaesthesia in sedated ponies undergoing field castration. Vet. Anaesth. Analg. 42(5), 512-517. Donaldson, L.L., Dunlop, G.S., Holland, M.S. and Burton, B.A. 2000. The recovery of horses from inhalant anesthesia: a comparison of halothane and isoflurane. Vet. Anesth. 29, 92-101. England, G.C.W. and Clarke, K.W. 1996. Alpha2 adrenoceptor agonists in the horse - a review. Br. Vet. J. 152, 641-657. England, G.C.W., Clarke, K.W. and Goossens, L. 1996. A comparison of the sedative effects of three alpha-2-adrenoceptor agonists (romifidine, detomidine and xylazine) in the horse. J. Vet. Pharmacol. Ther. 15(2), 194-201. Farmer, E., Chase-Topping, M., Lawson, H. and Clutton, R.E. 2014. Factors affecting the perception of recovery quality in horses after anaesthesia. Equine Vet. J. 46(3), 328-332. Harethardottir, H., Murison, P.J., Blissitt, K., Olason, S. and Clutton, R.E. 2019. A comparison of two ketamine doses for field anaesthesia in horses undergoing castration. Equine Vet. J. 51(4), 458-463. Kaka, J.S., Klavano, P.A. and Hayton, W.L. 1979. Pharmacokinetics of ketamine in the horse. Am. J. Vet. Res. 40(7), 978-981. Kerr, C.L., McDonnell, W.N. and Young, S.S. 1996. A comparison of romifidine and xylazine when used with diazepam/ketamine for short term anaesthesia in the horse. Can. Vet. J. 37, 601-609. Kloppel, H. and Leece, E.A. 2011. Comparison of ketamine and alfaxalone for induction and maintenance of anaesthesia in ponies undergoing castration. Vet. Anaesth. Analg. 38(1), 37-43. Larenza, M.P., Knobloch, M., Landoni, M.F., Levionnois, O.L., Kronen, P.W., Theurillat, R., Schatzmann, U. and Thormann, W. 2008. Stereoselective pharmacokinetics of ketamine and norketamine after racemic ketamine or S-ketamine administration in Shetland ponies sedated with xylazine. Vet. J. 177(3), 432-435. Lin, H.C., Passler, T., Wilborn, R.R., Taintor, J.S. and Caldwell, F.J. 2015. A review of the general pharmacology of ketamine and its clinical use for injectable anaesthesia in horses. Equine Vet. Ed. 27(3), 146-155. Marntell, S. and Nyman, G. 1996. Effects of additional premedication on romifidine and ketamine anaesthesia in horses. Acta Vet. Scand. 37, 315 - 325. Marntell, S., Nyman, G. and Funkquist, P. 2006. Dissociative anesthesia during field and hospital conditions for castration of colts. Acta Vet. Scand. 47, 1-11. Matthews, N.S., Hartsfield, S.M., Cornick, J.L., Williams, J.D. and Beasley, A. 1991. A comparison of injectable anesthetic combinations in the horse. Vet. Surg. 20(4), 268-273. Muir, W.W., Skarda, R.T. and Milne, D.W. 1977. Evaluation of xylazine and ketamine hydrochloride for anesthesia in horses. Am. J. Vet. Res. 38(2), 195-201. Peboni Figueiredo, J., Muir, W.W., Smith, J. and Wolfrom, G.W. 2005. Sedative and analgesic effects of romifidine in horses. Int. J. Appl. Res. Vet. Med. 3(3), 249-258. Price, J., Eager, R.A., Welsh, E.M. and Waran, N.K. 2005. Current practice relating to equine castration in the UK. Res. Vet. Sci. 78(3), 277-280. Rigotti, C., De Vries, A. and Taylor, P.M. 2014. Buprenorphine provides better anaesthetic conditions than butorphanol for field castration in ponies: results of a randomised clinical trial. Vet. Rec. 175(24), 623. Rossetti, R.B., Gaido Cortopassi, S.R., Intelizano, T., de Lima Machado, T.S. and Ferreira da Cruz, R.S. 2008. Comparison of ketamine and S(+)-ketamine, with romifidine and diazepam, for total intravenous anesthesia in horses. Vet. Anaesth. Analg. 35(1), 30-37. Smith, M.C., Bass, L., Damone, J., Mama, K. and Rao, S. 2020. Comparison of xylazine and detomidine in combination with midazolam/ketamine for field castration in Quarter Horses. Equine Vet. J. 52(4), 516-521. Taylor, P.M. and Clarke, K.W. 2007. Handbook of Equine Anaesthesia. Edinburgh: Saunders Elsevier. Waterman, A.E., Robertson, S.A. and Lane, J.G. 1987. Pharmacokinetics of intravenously administered ketamine in the horse. Res. Vet. Sci. 42(2), 162-166. Wojtasiak-Wypart, M., Soma, L.R., Rudy, J.A., Uboh, C.E., Boston, R.C. and Driessen, B. 2012. Pharmacokinetic profile and pharmacodynamic effects of romifidine hydrochloride in the horse. J. Vet. Pharmacol. Ther. 35(5), 478-488. Wright, M. 1982. Pharmacological effects of ketamine and its use in veterinary medicine. J. Am. Vet. Med. Assoc. 180(12), 1462-1471. Zoetis. 2021. Zoetis Ketavet(R) Datasheet [online]. Available at: https://www.noahcompendium.co.uk/?id=-457558 [Accessed 02/06/2021]. | ||
| How to Cite this Article |
| Pubmed Style Wise IK, Kloeppel H, Leece EA. Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. Open Vet. J.. 2021; 11(4): 747-754. doi:10.5455/OVJ.2021.v11.i4.27 Web Style Wise IK, Kloeppel H, Leece EA. Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. https://www.openveterinaryjournal.com/?mno=88610 [Access: January 25, 2026]. doi:10.5455/OVJ.2021.v11.i4.27 AMA (American Medical Association) Style Wise IK, Kloeppel H, Leece EA. Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. Open Vet. J.. 2021; 11(4): 747-754. doi:10.5455/OVJ.2021.v11.i4.27 Vancouver/ICMJE Style Wise IK, Kloeppel H, Leece EA. Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. Open Vet. J.. (2021), [cited January 25, 2026]; 11(4): 747-754. doi:10.5455/OVJ.2021.v11.i4.27 Harvard Style Wise, I. K., Kloeppel, . H. & Leece, . E. A. (2021) Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. Open Vet. J., 11 (4), 747-754. doi:10.5455/OVJ.2021.v11.i4.27 Turabian Style Wise, Innes K, Heide Kloeppel, and Elizabeth A Leece. 2021. Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. Open Veterinary Journal, 11 (4), 747-754. doi:10.5455/OVJ.2021.v11.i4.27 Chicago Style Wise, Innes K, Heide Kloeppel, and Elizabeth A Leece. "Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.." Open Veterinary Journal 11 (2021), 747-754. doi:10.5455/OVJ.2021.v11.i4.27 MLA (The Modern Language Association) Style Wise, Innes K, Heide Kloeppel, and Elizabeth A Leece. "Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.." Open Veterinary Journal 11.4 (2021), 747-754. Print. doi:10.5455/OVJ.2021.v11.i4.27 APA (American Psychological Association) Style Wise, I. K., Kloeppel, . H. & Leece, . E. A. (2021) Comparison of two doses of ketamine for induction of anaesthesia in ponies undergoing field castration.. Open Veterinary Journal, 11 (4), 747-754. doi:10.5455/OVJ.2021.v11.i4.27 |

