




| Research Article | ||
Open Vet. J.. 2024; 14(7): 1538-1552 Open Veterinary Journal, (2024), Vol. 14(7): 1538–1552 Research Article Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 casesRui Mizuno1 and Takashi Mori1,2*1Joint Graduate School of Veterinary Science, Gifu University, Gifu, Japan 2Animal Medical Center, Faculty of Applied Biological Sciences, Gifu University, Gifu, Japan *Corresponding Author: Takashi Mori. Animal Medical Center, Faculty of Applied Biological Sciences, Gifu University, Gifu, Japan. Email: tmori [at] gifu-u.ac.jp Submitted: 15/01/2024 Accepted: 27/06/2024 Published: 31/7/2024 © 2024 Open Veterinary Journal
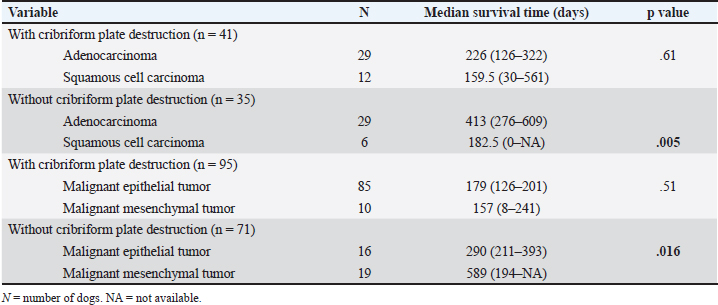
AbstractBackground: Prognostic factors in dogs with nasal tumors include several variables. However, factors that can measure prognosis have not yet been identified due to considerable divergence among reports. Aim: To describe the computed tomography (CT) imaging, treatment, and outcomes of dogs with nasal tumors, as well as detect negative prognostic factors through the analysis of a substantial number of cases from a single institution. Furthermore, based on CT findings, this study aimed to identify independent prognostic factors for nasal tumors in dogs. Methods: A total of 166 client-owned dogs were diagnosed with nasal tumors at Gifu University Veterinary Hospital between 2015 and 2019. Data were retrospectively collected from the electronic medical records. Results: Univariate analysis revealed a significant difference in survival time between adenocarcinoma and squamous cell carcinoma in 166 canine nasal tumors treated with megavoltage (MeV) radiation therapy at a single institution (p=.015). There was a significant difference in survival time between carcinoma and sarcoma (p=.04). Regarding CT imaging findings, significant differences in survival time were observed for frontal sinus invasion (p=.007), cribriform plate destruction (p < .001), and lymph node metastasis (p=.003). Multivariate Cox regression analysis was performed to assess frontal sinus invasion, cribriform plate destruction, histopathologic subtypes, and lymph node metastasis as negative prognostic factors; however, only cribriform plate destruction was a significant negative prognostic factor for survival time (p=.004). Conclusion: Multivariate Cox regression analysis showed that cribriform plate destruction was the main factor in predicting a negative prognosis among 166 canine nasal tumors treated with MeV radiation therapy at a single institution. Therefore, we propose a new 2-tier staging classification for canine nasal tumors with the presence or absence of cribriform plate destruction based on CT examination as the only evaluation factor. Keywords: Dog, Megavoltage radiation therapy, Metastasis, Nasal tumor, Prognostic factor. IntroductionSeveral variables have been described as having prognostic significance in dogs with nasal tumors. Negative survival prognostic factors from various studies include age >10 years (Ladue et al., 1999), epistaxis (Rassnick et al., 2006), duration of clinical signs (Gieger et al., 2008), advanced local tumor stage (Ladue et al., 1999; Adams et al., 2009; Buchholz et al., 2009), histopathologic subtype (carcinoma, particularly SCC of undifferentiated) (Adams et al., 2009; Buchholz et al., 2009), tumor expression of survivin (Fu et al., 2014), duration of clinical signs <90 days before diagnosis (Cancedda et al., 2015), and metastatic disease (Henry et al., 1998; Ladue et al., 1999; Cancedda et al., 2015). Lymph node and lung metastases have been reported as negative prognostic factors because they significantly shorten the survival time in other malignant tumors, such as oral malignant melanoma (Turek et al., 2020), mast cell tumors (Pecceu et al., 2020), lung histiocytic sarcoma (Marlowe et al., 2018), hemangiosarcoma (Alvarez et al., 2013), and osteosarcoma (Hillers et al., 2005). However, canine nasal tumors, in contrast to other malignant tumors, have been characterized by a reported low metastatic rate (Malinowski, 2006), and historically, metastatic status has not been considered important. Even in the modified Adams and computed tomography (CT) staging classifications, only local invasion is considered for staging because of the low distant metastasis rate. These staging systems, based on the CT findings, are categorized into 11 groups: unilateral or bilateral soft tissue lesions of the paranasal sinuses, frontal sinuses, orbit, skin, mucosa, nasopharynx, brain, bone destruction of the nasal septum, facial deformity, and cribriform plate destruction. These reports showed no significant differences in survival time at any stage; however, survival time was significantly shorter in stage 4, where cribriform plate destruction was observed (Adams et al., 1998, 2009; Kondo et al., 2008). Although cribriform plate destruction is a negative prognostic factor, the distance from the tumor to the cribriform plate and other factors have not yet been studied. The significance of prognostic factors in treating canine nasal tumors remains controversial. This may be due to the limited number of cases analyzed for prognostic factors, reliance on solely univariate analysis, and variations in case numbers among different institutions. Owing to the wide variation among reports, the prognostic factors reported in the past have not been widely accepted. This study aimed to determine positive prognostic factors for canine nasal tumors using the outcomes of 166 cases treated with megavoltage (MeV) radiation therapy. This is the largest cohort ever treated at a single institution. Materials and MethodsCriteria for selection of casesIn this retrospective study, the medical records of 166 dogs with malignant nasal tumors who underwent CT and MeV radiation therapy were reviewed. The patients were treated at the Oncology Services of Gifu University Veterinary Medical Hospital between January 2015 and December 2019. Histological diagnosis was established through tissue specimens obtained during tissue biopsy using a plastic cannula or by cytology of the nasal cavity immediately after CT. For each patient eligible for study inclusion, information extracted from electronic medical records included signalment (age, breed, sex, neuter status, and body weight), histopathological subtypes, various treatments (MeV radiation therapy with or without chemotherapy), and follow-up information regarding the cause of death. The starting point of the overall survival time was the date of treatment initiation, and the endpoint was determined by death from any cause (including euthanasia) or confirmation of death through communication with the home doctor. Cases without available prognostic studies were considered censored (22 censored cases). The breakdown of causes of death included 108 deaths related to tumors, eight deaths due to other causes (such as tumors in areas other than the nasal cavity, chronic diseases, and so on), three deaths due to senility, 43 deaths of unknown cause (not documented in medical records, including censored cases), and four cases of euthanasia. Euthanasia was performed in four cases; all four had recurrent tumors and a worsening general condition. Owners were informed about the prognosis and the maximum potential palliative treatment. Euthanasia was carried out in a humane manner based on the owner's request, considering the owner's wishes, the animal's general condition, and the available treatment options. ImagingCT was performed for tumor staging and treatment planning in all dogs. CT imaging was evaluated at six sites of osteolysis (nasal septum, plate, orbit, frontal bone, cribriform plate, and cranium) and eight sites of invasion (unilateral or bilateral, nasal septum, oral cavity, orbit, frontal sinus, forehead, nasopharynx, and brain). The distance between the tumor and the cribriform plate was measured using three-dimensional multiplanar reconstruction of the head CT images. A line was drawn along the cribriform plate on the sagittal and horizontal cross-sectional images, representing the location of the cribriform plate. Subsequently, a vertical line was drawn vertically across the cribriform plate from the proximal side of the tumor, and this distance was considered the measurement between the tumor and the cribriform plate. Radiation morbidity was scored based on the VRTOG grade (LaDue and Klein, 2001). Volume measurements were conducted by a single author using an open-source image analysis software called Horos version 3. The nasal tumors were measured using a closed polygon region of interest on each 2 mm CT slice throughout the entire nasal cavity, using both pre- and post-radiotherapy CT scans. All CT scans with 2 mm slice thickness were performed using the same scanner (Aquilion 16 CT, Canon Medical Systems Corporation, Tochigi, Japan). Metastases in the mandibular and medial retropharyngeal lymph nodes, as well as the lungs, were evaluated. Lymph node size was considered metastatic if it measured ≥10 mm in length and width. Pulmonary metastasis was determined by the presence of either solitary or multiple lesions. Statistical analysisStatistical analyses were performed using the statistical software R. Survival curves were generated using the Kaplan–Meier method, which accounted for (i.e., censored) dogs that had been lost to follow-up, and the log-rank test and multivariate Cox regression analysis were used for correlation analysis. A paired t-test was used to compare the rates of tumor volume reduction. Statistical significance was set at p < .05. Ethical approvalNo laboratory animals were used in this study; only data from domestic animals that were admitted to the Oncology Services of Gifu University Veterinary Medical Hospital were used. Informed consent was obtained from the owners after explaining the background of the nasal tumor and the maximum possible treatment; the agreed-upon maximum possible treatment was administered. ResultsBreed, sex, average weight, and average age of dogs used in the studyThe medical data of 166 dogs were analyzed. Of these, 153 (92.2%) were purebred and 13 (7.8%) were mixed breeds. The purebred dogs included 23 miniature Dachshunds, 21 Shibas, 16 Pembroke Welsh Corgis, 12 Toy Poodles, 10 golden retrievers, and 10 Labrador retrievers. The remaining breeds, each with smaller numbers, were Shetland sheepdogs, Papillons, Chihuahuas, beagles, Pomeranians, Miniature Schnauzers, Yorkshire terriers, Border Collies, Jack Russell Terriers, Irish setters, Cavalier King Charles Spaniels, French bulldogs, English Cocker Spaniels, Italian Greyhounds, Cairn terriers, Collies, Shih Tzus, German shepherds, Siberian huskies, Staffordshire Bull Terriers, Scottish Terriers, Chinese crested dogs, Bernese mountain dogs, Flat-Coated Retrievers, and Akitas. Thirty-six of the dogs were male, 53 of which were neutered, while 26 were female, with 51 being spayed. The average age and body weight were 11.12 years (range: 3 to 16 years) and 12.72 kg (range: 1.84 to 58.5 kg), respectively. Univariate analysis of histopathologic subtypes and survival timeThe histopathological results are presented in Table 1. A significant difference in survival time was observed between adenocarcinoma (311 days) and squamous cell carcinoma (162.5 days; p=.015). Additionally, there was a significant difference in the survival time of dogs with 140 malignant epithelial tumors (207 days) and 26 malignant mesenchymal tumors (250 days; p=.04). Among cases with adenocarcinoma and squamous cell carcinoma, we performed analysis in 41 cases with cribriform plate destruction and 35 cases without cribriform plate destruction. In the group with cribriform plate destruction, there was no significant difference in survival time between 29 adenocarcinomas (226 days) and 12 squamous cell carcinomas (159.5 days) (p=.61). In the group without cribriform plate destruction, there was a significant difference in survival time between 29 adenocarcinomas (413 days) and six squamous cell carcinomas (182.5 days) (p=.005). Table 1. Histopathology results (N=166).
In addition, there was no significant difference in survival time when comparing 95 dogs with malignant epithelial tumors (85 dogs; 179 days) and 10 dogs with malignant mesenchymal tumors (157 days) in whom cribriform plate destruction was observed (p=.51). However, in 71 dogs without cribriform plate destruction, when comparing 55 malignant epithelial tumors (290 days) and 16 malignant mesenchymal tumors (589 days), there was a significant difference in the survival time (p=.016; Table 2). Univariate analysis of irradiation protocol and survival timeThe median irradiation dose/fraction was 7 Gy (range: 2.5–14 Gy); the median total dose was 48 Gy (range: 4–60 Gy). The median daily radiation dose was 14.29 (range: 5%–100%). There were three cases where dogs were irradiated at a rate of 100% per day, and one dog was only irradiated once due to deterioration of its condition. Additionally, two patients died immediately after irradiation. The median number of irradiation fractions was 7 times (range: 1–20 times). The median duration of treatment was 40 days (range: 1–99 days). One case required 99 days to complete irradiation due to illness immediately after the treatment. The median survival time for all dogs was 198 days (range: 0–1505 days). There was no significant difference in survival between the different radiation modalities (1–5 times per week) (p=.52). Patients were classified into six groups based on improvement in clinical signs from the start of treatment. Symptoms completely resolved in 86 cases, with a median time of 21 days for symptom resolution (range: 1–154 days). In 49 cases, symptoms decreased but remained, and the date of the last hospital visit was considered the date when symptoms remained. The median duration for these cases was 52 days (range: 15–350 days). There were two cases with no change, three cases of worsening, and 3 cases with an unknown outcome (Table 3). Recurrence was confirmed in 69 out of 166 cases, and in 97 cases it was unknown. Among these, we studied 40 cases that experienced complete resolution of symptoms, as well as 19 cases with reduced but residual symptoms. The median overall survival time for these 59 cases was 201 days (range: 66–1505 days), with a median time to improvement of 28 days (range: 1–162 days) and a median progression-free survival time of 84 days (range: 1–751 days). There were no significant differences in time to improvement, progression-free survival time, or overall survival time between the 37 cases in the radiation therapy and chemotherapy group and the 20 cases in the chemotherapy-naive group (p=.098, .11, and .78). The number of weekly fractions used for radiation therapy was compared. In 52 cases, radiation therapy was administered once per week, while in four cases it was administered three times per week, and in three cases it was administered five times per week. There were no cases in which radiation therapy was administered twice per week or four times per week in either group. A significant difference was found in the median time to improvement and overall survival between the once-weekly and three times-weekly irradiation groups (p=.017, p=.023). However, since the number of cases receiving three times-weekly irradiation was very small (four cases), this finding is still subject to debate and further cases need to be included. No differences were observed between the irradiation methods in any other conditions (Table 4). Table 2. Univariate analysis of the relationship between histopathological subtype and survival with or without cribriform plate destruction (n=95).
Table 3. Median time to clinical sign improvement after treatment in dogs with nasal tumors.
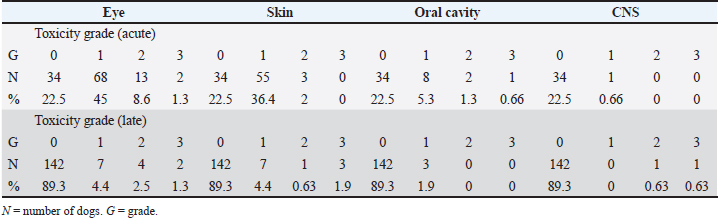
Univariate analysis of irradiation morbidity score and survival timeOf the 166 cases, 151 had documented acute radiation side effects in the medical record, with 15 cases having unknown side effects. Out of the 17 cases with late side effects, seven cases had unknown side effects. No entries were allowed in the medical record. For the 142 cases that were not documented in the medical record, it was concluded that no late radiation side effects occurred. The VRTOG score was used to evaluate radiation side effects, and a breakdown of these scores is presented in Table 5. The survival time was compared between cases with early and late radiation side effects. Radiation side effects were assessed based on the VRTOG grade, considering all grades of disability that actually occurred. There was no significant difference between the radiation side effect score and survival time (Table 6; p=.17). Out of the 151 cases with early and late radiation side effects out of 166 cases, survival time was examined in 30 cases with no radiation side effects, 106 cases with early radiation side effects, and 15 cases with late radiation side effects. A significantly prolonged survival time was observed in cases of late radiation side effects (p=.025; Table 7). Univariate analysis of tumor reduction rate and histopathologic subtypeThe rate of reduction of nasal tumors in dogs, resulting from MeV radiation therapy, was calculated using 150 out of 166 cases in which the effects before and after treatment were confirmed by CT scan. The details are presented in Table 8. Malignant epithelial tumors showed a tendency to have a higher reduction rate with MeV radiation therapy compared to malignant mesenchymal tumors. However, there was no significant difference the between histopathologic subtype and the rate of tumor reduction with MeV radiation therapy (p=.176). Table 4. Impact of each treatment modality on time to clinical sign improvement, progression-free days, and overall survival time in canine nasal tumors.
Table 5. Veterinary radiation therapy oncology group (VRTOG) scores expressed as cases for canine nasal tumor dogs treated with MeV radiation therapy.
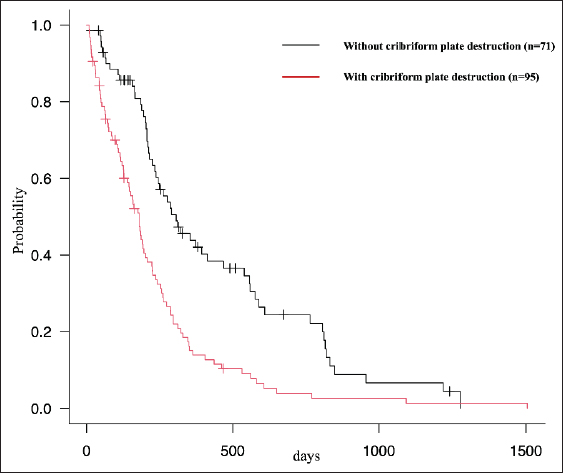
Univariate analysis of chemotherapy and survival timeForty-three dogs received combined radiation therapy and chemotherapy, but there was no significant difference in survival time between the 123 dogs who did not receive chemotherapy and the 43 dogs who did (p=.145). Combined treatments with and without cribriform plate destruction were examined, but neither showed a significant difference in survival time (p=.05, cribriform plate destruction; p=.54, without cribriform plate destruction). Bone invasion sites and survival time Univariate analysisSix sites of bone invasion were examined: the nasal septum, palate, orbit, frontal bone, cribriform plate, and cranium. Significant differences in survival time were observed for frontal bone invasion (p=.001) and cribriform plate destruction (p < .001; Table 9). The survival time for cribriform plate destruction is shown in Figure 1. Multivariate Cox regression analysisAmong the six bone invasion sites, only cribriform plate destruction was significantly different as a negative prognostic factor for survival time (p < .001). Soft tissue invasion sites and survival time Univariate analysisEight sites of soft tissue invasion were considered: unilateral or bilateral, the nasal septum, oral cavity, orbit, frontal sinus, forehead, nasopharynx, and brain. Significant differences in survival times were observed for brain invasion (p=.004), frontal sinus invasion (p=.007), and orbital invasion (p=.002; Table 9). Table 6. Radiation morbidity scoring and median survival time for canine nasal tumor dogs treated with MeV radiation therapy.
Table 7. Radiation side effects and median survival time.
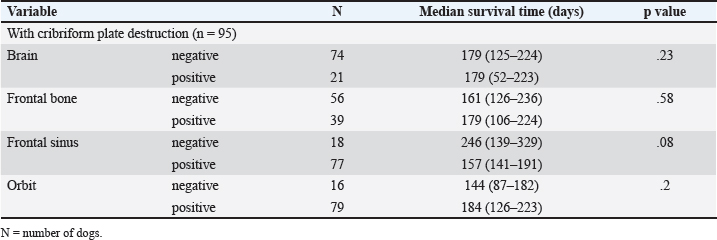
Of the 166 cases, cribriform plate destruction was observed in 95 cases and brain invasion in 21 cases. All cases of brain invasion showed cribriform plate destruction. Of the 95 cases with cribriform plate destruction, no significant difference was observed in survival time between the 74 cases without and the 21 cases with brain invasion. We also examined frontal bone, frontal sinus, and orbital invasion in 95 cases with cribriform plate destruction, none showing significant differences in survival times (Table 10). Multivariate Cox regression analysisAmong the eight soft tissue invasion sites, only frontal sinus invasion was significantly different as a negative prognostic factor for survival time (p=.007; Table 11). Univariate analysis of the distance between the tumor and the cribriform plate and survival timeThe median distance between the tumor and cribriform plate was 20.05 mm (range: 0–79.3 mm). In total, 95 dogs with cribriform plate destruction, 54 dogs without cribriform plate destruction but with tumors in contact with the cribriform plate, eight dogs with a distance from the cribriform plate of less than 20 mm, and nine dogs with tumors larger than 20 mm were compared. There was a significantly shorter survival time in the group with cribriform plate destruction compared to the other groups (p=.002; Fig. 2). The groups without cribriform plate destruction were also examined, but no significant difference in survival time was found based on the distance between the tumor and the cribriform plate (p=.39). Univariate analysis of metastasis and survival timeMetastasis was observed in 19 dogs (11.4%) out of the 166. Lymph node metastasis was defined by a short and long diameter of 10 mm, given the significant differences in lymph node size and survival time observed at 10 mm on CT images (Table 12). Among the metastatic cases, 12 dogs had only lymph node metastases, six had only lung metastases, and one had both. There was a significant difference in survival between dogs with lymph node metastasis (126 days) and those without (226 days, p=.003), as illustrated in Figure 3. However, there was no significant difference in survival time between those without lymph node metastasis and those with lymph node metastasis (p=.7). Table 8. Evaluation of tumor volume reduction of nasal malignant epithelial tumors versus malignant mesenchymal tumors in dogs treated with MeV radiation therapy.
Table 9. Variables demonstrating a statistically significantly relationship with survival time in the univariate analysis.
Among the 95 dogs with cribriform plate destruction, no significant differences in survival time were found between the 85 dogs without metastases (182 days) and the 10 dogs with metastases (125 days) (p=.242). In the 71 dogs without cribriform plate destruction, a significant difference in survival time (p=.002) was observed when comparing 68 dogs without metastasis (311 days) and three dogs with metastasis (164 days). Multivariate Cox regression analysis of frontal sinus invasion, cribriform plate destruction, histopathologic subtypes, and lymph node metastasis and survival timeThe results are summarized in Table 13. Analysis of negative prognostic factors in 166 dogs with nasal tumors treated with MeV radiation therapy revealed that only cribriform plate destruction was a significant negative prognostic factor for survival (p=.004). DiscussionMedical records of 166 dogs with nasal tumors treated with MeV radiation therapy were retrospectively reviewed. Univariate and multivariate Cox regression analyses revealed five negative prognostic factors: frontal sinus invasion, cribriform plate destruction, histopathological subtypes, and metastases. However, when multivariate Cox regression analysis was performed on these five negative prognostic factors, only cribriform plate destruction was found to be a negative prognostic factor.
Fig. 1. Survival time of dogs with or without cribriform plate destruction (2-tier staging system for canine nasal tumors). The dogs with cribriform plate destruction had a significantly shorter survival time than those without (MST, 179 days, 306 days, p=.0001). Table 10. Univariate analysis of the relationship between brain, frontal bone, frontal sinus, and orbital invasion and survival with cribriform plate destruction (n=95).
Tumor (degree of progression, histopathological subtype, and metastasis) and treatment (surgical treatment, radiation therapy, chemotherapy, and combination therapy) factors have been reported as prognostic factors for canine nasal tumors. In this study, MeV radiotherapy was administered, and no significant difference in survival time was found between irradiation protocols or with and without chemotherapy as a treatment factor. Some reports suggest that a hyperfractionated irradiation protocol can prolong survival (Adams et al., 1998, 2005, 2009; Lana et al., 2004; Lawrence et al., 2010). There was a significant difference observed in the median time to improvement and overall survival when comparing once-weekly and three times-weekly irradiations (p=.017 and p=.023). However, due to the limited number of cases (only four) that received three times-weekly irradiation, the significance of the findings is still debatable. Therefore, there is a need to increase the number of cases to further investigate this difference. The notable variation in the number of cases resulting from the large number of weekly irradiation protocols in our study (140 cases) and the advanced stage of cribriform plate destruction may have contributed to differences in survival time. In 151 cases with confirmed radiation side effects, the survival time was compared in three groups: 30 cases without radiation side effects, 106 cases with early radiation side effects, and 15 cases with late radiation side effects. There was a significant survival time benefit in the group with late radiation side effects. However, this result was based on the fact that in all cases where late radiation side effects were observed, they occurred more than six months after the onset of the disorder. This was considered a natural result since late radiation side effects are disorders that should only be recognized due to prolonged survival time. There was no significant difference in the rate of reduction between malignant epithelial and malignant mesenchymal tumors in nasal tumor reduction in dogs treated with MeV radiation therapy. However, malignant epithelial tumors tended to show a higher rate of tumor shrinkage compared to malignant mesenchymal tumors. Morgan et al. (2018) reported that malignant epithelial tumors exhibited a significant tumor reduction rate compared to malignant mesenchymal tumors, suggesting the involvement of the α/β ratio based on tumor histopathologic subtypes. In canine osteosarcoma cell lines, which are malignant mesenchymal tumors, the α/β ratio is low (Fitzpatrick et al., 2008). In humans, α/β ratios are high in malignant epithelial tumors such as squamous cell carcinoma, transitional cell carcinoma, basal cell carcinoma, and non-small cell lung cancer, but low in breast and prostate cancer. Both the tumor site and histologic type have been reported as important factors in the α/β ratio (Leeuwen et al., 2018). When using a low α/β ratio in radiation biology, the effect increases as the once-per-line dose increases. In this study, we compared the tumor reduction rate in 150 cases. Of these, 19 cases underwent fractionated irradiation twice to five times a week for malignant epithelial tumors, while 17 cases received irradiation once a week for malignant mesenchymal tumors. No significant difference in reduction rate was found (p=.286). These results suggest that dogs with nasal tumors of malignant epithelial origin are more sensitive to MeV radiation therapy compared to malignant mesenchymal tumors. However, considering the incidence rate of histopathologic subtypes in this study, the large difference in the number of cases does not appear to be significant. Table 11. Multivariate analysis of bone and soft tissue invasion sites.
Fig. 2. A significant reduction in survival time within the group exhibiting cribriform plate destruction compared to the other groups (179 days vs. 311 days, 244.5 days, 214 days, p=.002). Table 12. Univariate analysis for lymph node size on survival time.
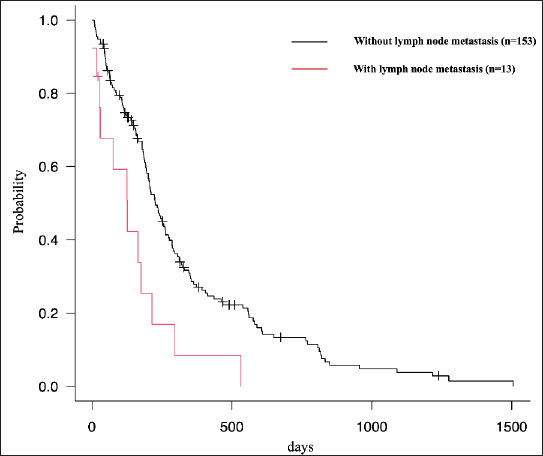
Fig. 3. Presence of lymph node metastasis in 13 dogs. A significant difference in survival time was observed in those with (MST, 126 days) or without lymph node metastasis (MST, 226 days, p=.003). Table 13. Multivariate analysis of negative prognostic factors in dogs with intranasal tumors treated using radiation therapy (n=166).
Although some reports suggest the efficacy of chemotherapy, either in combination or alone (Lana et al., 1997, 2004; Langova et al., 2004), making comparisons is challenging due to the limited number of reports and cases. While there was no clear efficacy observed in this study, there was a trend towards prolonged survival time with combined chemotherapy in the group with cribriform plate destruction. In the group without cribriform plate destruction, combined chemotherapy had no effect on survival time. Similarly, it was not possible to conclusively demonstrate the ineffectiveness of chemotherapy due to the small number of cases. The modified adams clinical staging method and CT staging, which are currently validated staging methods for canine nasal tumors, are CT-based classifications. Nasal tumors are staged according to the evaluation of 11 local invasions: unilateral or bilateral soft tissue involvement of the paranasal sinuses, frontal sinuses, orbit, skin, mucosa, nasopharynx, and brain; bone destruction of the nasal septum; facial deformity; and cribriform plate destruction (Adams et al., 1998, 2009; Kondo et al., 2008). We examined 14 sites, including six bone invasion sites and eight soft tissue invasion sites, including previously evaluated sites. In the univariate analysis of bone and soft tissue invasion sites, significant differences in survival time were observed between frontal bone invasion (p=.001) and cribriform plate destruction (p < .001). For soft tissue invasion, significant differences in survival times were observed for brain (p=.004), frontal sinus (p=.007), and orbital (p=.002) invasion. Multivariate Cox regression analysis was performed for the bone and soft tissue invasion sites, and significant differences were found only for cribriform plate destruction and frontal sinus invasion. Interestingly, in patients with cribriform plate destruction, there was no significant difference in the survival time for brain, frontal bone, frontal sinus, or orbital invasion. Multivariate Cox regression analysis revealed a significant difference in survival time only for cribriform plate destruction at the site of bone invasion. Thus, because it is the strongest prognostic factor, other prognostic factors may not function in the presence of cribriform plate destruction. Stage 4 in the modified adams clinical staging method and stage 4 of CT staging differed in their classifications. Stage 4 of the modified Adams clinical staging method includes only cribriform plate destruction, whereas stage 4 of CT staging is classified by considering not only cribriform plate destruction but also brain invasion (Adams et al., 1998, 2009; Kondo et al., 2008). In our study, 95/166 cases of cribriform plate destruction and 21/166 cases of brain invasion were considered factors for classification as stage 4. Cribriform plate destruction was observed in all the cases of brain invasion. Of the 95 cases with cribriform plate destruction, no significant difference in survival time was observed between the 74 cases without brain invasion and the 21 cases with brain invasion (p=.232). Although cribriform plate destruction and brain invasion showed significant differences in survival time in the univariate analysis, it is difficult to imagine brain invasion occurring without cribriform plate destruction. In addition, brain invasion is a weak negative prognostic factor in the presence of cribriform plate destruction. Thus, although cribriform plate destruction should be considered during staging, brain invasion is less likely. In addition, the distance between the tumor and the cribriform plate was measured, and the relationship between the distance and survival time was examined. A median distance of 20 mm was used as the baseline. There was no significant difference in survival time based on the distance between the tumor and the cribriform plate. The limited number of cases with clearly measured distance between the cribriform plate and tumor (17 cases, eight with a distance less than 20 mm and nine with a distance more than 20 mm) hindered a comprehensive analysis. Additionally, in 54 cases, there was no cribriform plate destruction, but the cribriform plate was in contact with the tumor. Distinguishing between a tumor and an effusion secondary to the tumor on CT was challenging. While MRI has been reported to be more sensitive in detecting small fluid retention in canine nasal tumors, no difference in evaluating tumor invasion between CT and MRI was observed when the tumor was confined to the nasal cavity without intracranial invasion (Drees et al., 2009). Prolonging survival time may be associated with the time until cribriform plate destruction occurs, as it is a negative prognostic factor. However, there was no significant difference in survival time based on the distance between the tumor and the cribriform plate destruction. This could be influenced by variable growth rates associated with histopathological subtype and tumor location, which may lead to variations in the data and make it less likely to be a prognostic factor. In addition, since many of the cases in our study were in the end stages of the disease, the number of cases in which the distance between the tumor and cribriform plate could be measured was small and thus not sufficiently analyzed. Significant variations in survival times between the histopathological subtypes have been reported (Malinowski, 2006; Adams et al., 2009). In this study, the survival time was significantly shorter for malignant epithelial tumors, especially squamous cell carcinoma (162.5 days, p=.01), consistent with previous reports (Henry et al., 1998; Adams et al., 2009). There was also a significant difference in the survival time between malignant epithelial and mesenchymal tumors (p=.04). While various reports have highlighted differences in survival time between patients with epithelial and mesenchymal tumors (Malinowski, 2006; Adams et al., 2009), these findings are based on univariate analysis. We considered histopathological subtypes as negative prognostic factors and performed a multivariate Cox regression analysis, which showed no significant differences. The effect of histopathological subtypes on survival, analyzed in 166 dogs, varied significantly between those with and without cribriform plate destruction. In the presence of cribriform plate destruction, there was no significant difference in the survival time between the histopathological subtypes; however, in the absence of cribriform plate disruption, a significant difference in survival time was observed between the histopathological subtypes. In our study, we found that squamous cell carcinoma had a significantly shorter survival time compared to adenocarcinoma in the group of dogs without cribriform plate destruction. While there are few reports that have investigated the differences in survival time between histopathologic subtypes (Stevens et al., 2020; Czichon et al., 2022; Yoshikawa et al., 2023), these reports did not take into account the presence of cribriform plate destruction. We observed a median survival time of 165 days (range: 30–330 days) in six dogs treated with cobalt-60 radiation therapy for intranasal squamous cell carcinoma without cribriform plate destruction. It is worth noting that squamous cell carcinoma is known to be less responsive to radiation therapy (Correa et al., 2003). Another study examined cobalt-60 radiation therapy in 21 dogs with nasal malignancies. The researchers selected 11 dogs with malignant epithelial tumors, excluding cases with cribriform plate destruction and squamous cell carcinoma, to match their report. The median survival time in this group was found to be 410 days (range: 120–1800 days) (Adams et al., 1998). Comparing these reports, it appears that in the group without cribriform plate destruction, squamous cell carcinoma had a shorter survival time than other malignant epithelial tumors. This is likely because it was less responsive to radiation therapy. Additionally, squamous cell carcinomas had a lower response rate to orthovoltage radiation therapy compared to other malignant epithelial tumors. They also had the lowest median survival rate in comparison, although it is not clear whether cribriform plate destruction was present (Fu et al., 2014). To further validate the effectiveness of radiation therapy, we compared the tumor volume reduction rates of 25 adenocarcinomas and 6 squamous cell carcinomas out of 31 dogs without cribriform plate destruction. We confirmed the changes in tumor volume after radiation therapy and found no significant difference in the reduction rate (p=.646). The median disease-free period was compared between 13 cases of adenocarcinoma and three cases of squamous cell carcinoma. In these cases, where there was no cribriform plate destruction and the disease-free interval after radiation therapy could be calculated, the disease-free interval was significantly shorter in squamous cell carcinoma compared to adenocarcinoma (284 days for adenocarcinoma, 41 days for squamous cell carcinoma; p=.024). These findings suggest that, in the absence of cribriform plate destruction, squamous cell carcinoma exhibits a similar response to radiation therapy in terms of tumor reduction compared to adenocarcinoma. However, squamous cell carcinoma is associated with a shorter disease-free interval, indicating a shorter survival time due to a higher likelihood of recurrence. It should be noted that the number of cases in this study is very small, and further accumulation of cases is necessary to strengthen these observations. These results suggest that cribriform plate destruction is the strongest negative prognostic factor. Thus, in the presence of cribriform plate destruction, local invasion of other sites, histopathological subtypes, and metastases may have no prognostic effect. Various studies have reported that metastasis is not a negative prognostic factor in canine nasal tumors (Cancedda et al., 2015; Bowles et al., 2016) but is a prognostic factor (Henry et al., 1998; Ladue et al., 1999). Even if metastasis is considered a prognostic factor, these results are predominantly based on univariate analyses (Henry et al., 1998; Ladue et al., 1999). In addition, the term "metastasis" varies across reports, ranging from lymph node metastasis alone (Ladue et al., 1999) to combinations of lymph node and lung metastasis (Henry et al., 1998). Some reports (Mason et al., 2013) have described several cases but have not examined the prognostic factors. We obtained data on lymph node and lung metastasis rates from previous reports, revealing a lymph node metastasis rate ranging from 0% to 18.8% and a lung metastasis rate ranging from 0% to 11.9% (Adams et al., 1998; Henry et al., 1998; Ladue et al., 1999; Northrup et al., 2001; Langova et al., 2004; Rassnick et al., 2006; Gieger et al., 2008; Buchholz et al., 2009; Maruo et al., 2011; Mason et al., 2013; Gieger et al., 2013; Fu et al., 2014; Cancedda et al., 2015; Bowles et al., 2016; Gieger et al., 2017). Our study found that lymph node metastasis was approximately 1.9 times more common than lung metastasis, with a lymph node metastasis rate of 7.8% and a lung metastasis rate of 4.2%. Survival time was assessed by grouping lymph node sizes between 5 and 15 mm at 1 mm intervals, revealing significant differences in survival time for lymph node sizes greater than 10 mm. Thus, lymph node metastasis was considered present if the size of the lymph node exceeded 10 mm in both the short and long diameters on the CT scan. Univariate analysis indicated a significant difference in survival for lymph node metastases but not for lung metastases. Lymph node metastasis was not significantly different in the multivariate Cox regression analysis, although significant differences in survival time were found in the univariate analysis. The presence of metastasis was also examined using cribriform plate destruction, and there was no significant difference in survival time. However, when examining the presence or absence of metastasis without cribriform plate destruction, a significant difference in the survival time was observed, although the number of patients with metastasis was small. In conclusion, the multivariate Cox regression analysis results suggested that lymph node metastasis was not a negative prognostic factor because cribriform plate destruction was an overwhelmingly significant negative prognostic factor. We also attempted to compare our findings with previous reports where the presence of lymph node metastasis was considered a negative prognostic factor (Henry et al., 1998; Ladue et al., 1999) and those where it was not considered as such (Cancedda et al., 2015; Bowles et al., 2016). However, the former studies utilized the World Health Organization classification, while the staging criteria in the latter were unclear. As a result, we could not determine the number of cases with cribriform plate destruction. Based on these findings, a multivariate Cox regression analysis was conducted to assess histopathological subtypes, cribriform plate destruction, frontal sinus invasion, and lymph node metastasis as negative prognostic factors. Cribriform plate destruction was found to be a negative prognostic factor. Our study extensively examined the association of inferred prognostic factors in canine nasal tumors, considering not only individual assessments through univariate analysis but also a comprehensive multivariate Cox regression analysis. These results underscore that cribriform plate destruction stands out as the most substantial negative prognostic factor, suggesting that in the presence of cribriform plate destruction, factors such as local invasion of other sites, histopathological subtypes, and even metastases may have no prognostic impact. A limitation of this study was that lymph node biopsies were not performed on all dogs. The presence of metastasis was estimated using lymph nodes larger than 10 mm on CT images. The disadvantage of this approach is that a biopsy is not performed; therefore, there is a risk that hyperplasia may be included, and lymph node metastases may be overestimated. Various prognostically negative tumor factors and prognostically positive treatment factors have been reported, mostly using univariate analyses. In this study, there were no significant differences in survival time among the treatment factors; however, there were significant differences in survival time among the tumor factors (degree of progression, pathological subtype, and metastasis). In particular, a complex combination of various negative prognostic factors likely influences the prognosis of canine nasal tumors. Therefore, this study utilized 166 dogs diagnosed with nasal tumors and treated with MeV radiation therapy to individually examine each prognostic factor. Considering these associations, the multivariate Cox regression analysis revealed that the main factor in predicting a negative prognosis was cribriform plate destruction. In this retrospective study analyzing the medical records of 166 dogs with nasal tumors treated using MeV radiation therapy, only cribriform plate destruction emerged as a robust negative prognostic factor. Four staging classifications for canine nasal tumors have been proposed, including the CT-based Modified Adams Clinical Staging Method and CT staging. However, numerous complicated evaluation items may lead to variations among diagnostic physicians. We also examined several negative prognostic factors, including those reported previously, and found that cribriform plate destruction was the main factor in predicting a negative prognosis. Therefore, based on the results of the present study, we propose a new 2-tier staging classification for canine nasal tumors with the presence or absence of cribriform plate destruction based on CT examination as the only evaluation factor (Fig. 1). AcknowledgmentsNot applicable. Conflict of interestThe authors declare that there is no conflict of interest. Authors’ contributionsTakashi Mori conceived the study, and Rui Mizuno wrote the manuscript. FundingThis research received no specific grant. Data availabilityAll data supporting the findings of this study are available within the manuscript. ReferencesAdams, W.M., Bjorling, D.E., McAnulty, J.F., Green, E.M., Forrest, L.J. and Vail, D.M. 2005. Outcome of accelerated radiotherapy alone or accelerated radiotherapy followed by exenteration of the nasal cavity in dogs with intranasal neoplasia: 53 cases (1990-2002). JAVMA. 227, 936–941. Adams, W.M., Kleiter, M.M., Thrall, D.E., Klauer, J.M., Forrest, L.J., La Due, T.A. and Havighurst, T.C. 2009. Prognostic significance of tumor histology and computed tomographic staging for radiation treatment response of canine nasal tumors. Vet. Radiol. Ultrasound. 50, 330–335. Adams, W.M., Miller, P.E., Vail, D.M., Forrest, L.J. and MacEwen, E.G. 1998. An accelerated technique for irradiation of malignant canine nasal and paranasal sinus tumors. Vet. Radiol. Ultrasound. 39, 475–481. Alvarez, F.J., Hosoya, K., Lara-Garcia, A., Kisseberth, W. and Couto, G. 2013. VAC protocol for treatment of dogs with Stage III hemangiosarcoma. J. Am. Anim. Hosp. Assoc. 49, 370–377. Bowles, K., DeSandre-Robinson, D., Kubicek, L., Lurie, D., Milner, R. and Boston, S.E. 2016. Outcome of definitive fractionated radiation followed by exenteration of the nasal cavity in dogs with sinonasal neoplasia: 16 cases. Vet. Comp. Oncol. 14, 350–360. Buchholz, J., Hagen, R., Leo, C., Ebling, A., Roos, M., Kaser-Hotz, B. and Bley, C.R. 2009. 3D conformal radiation therapy for palliative treatment of canine nasal tumors. Vet. Radiol. Ultrasound. 50, 679–683. Cancedda, S., Sabattini, S., Bettini, G., Leone, V.F., Laganga, P., Rossi, F., Terragni, R., Gnudi, G. and Vignoli, M. 2015. Combination of radiation therapy and firocoxib for the treatment of canine nasal carcinoma. Vet. Radiol. Ultrasound. 56, 335–343. Correa, S.S., Mauldin, G.N., Mauldin, G.E. and Patnaik, A.K. 2003. Efficacy of Cobalt-60 radiation therapy for the treatment of nasal cavity nonkeratinizing squamous cell carcinoma in the dog. J. Am. Anim. Hosp. Assoc. 39, 86–89. Czichon, F., Bley, C.R. and Meier, V. 2022. Relative tumor volume has prognostic relevance in canine sinonasal tumors treated with radiation therapy: a retrospective study. PLoS One 17, 1–14. Drees, R., Forrest, L.J. and Chappell, R. 2009. Comparison of computed tomography and magnetic resonance imaging for the evaluation of canine intranasal neoplasia. J. Small Anim. Pract. 50, 334–340. Fitzpatrick, C.L., Farese, J.P., Milner, R.J., Salute, M.E., Rajon, D.A., Morris, C.G., Bova, F.J., Lurie, D.M. and Siemann, D.W. 2008. Intrinsic radiosensitivity and repair of sublethal radiation-induced damage in canine osteosarcoma cell lines. Am. J. Vet. Res. 69, 1197–1202. Fu, D.R., Kato, D., Watabe, A., Endo, Y. and Kadosawa, T. 2014. Prognostic utility of apoptosis index, Ki-67 and survivin expression in dogs with nasal carcinoma treated with orthovoltage radiation therapy. J. Vet. Med. Sci. 76, 1505–1512. Gieger, T., Rassnick, K., Siegel, S., Proulx, D., Bergman, P., Anderson, C., LaDue, T., Smith, A., Northrup, N. and Roberts, R. 2008. Palliation of clinical signs in 48 dogs with nasal carcinomas treated with coarse-fraction radiation therapy. J. Am. Anim. Hosp. Assoc. 44, 116–123. Gieger, T., Siegel, S., Rosen, K., Jackson, D., Ware, K., Kiselow, M. and Shiomitsu, K. 2013. Reirradiation of canine nasal carcinomas treated with coarsely fractionated radiation protocols: 37 cases. J. Am. Anim. Hosp. Assoc. 49, 318–324. Gieger, T.L. and Nolan, M.W. 2017. Linac-based stereotactic radiation therapy for canine non-lymphomatous nasal tumours: 29 cases (2013–2016). Vet. Comp. Oncol. 16, E68–E75. Henry, C.J., Brewer, W.G., Tyler, J.W., Brawner, W.R., Henderson, R.A., Hankes, G.H. and Royer, N. 1998. Survival in dogs with nasal adenocarcinoma: 64 cases (1981–1995). J. Vet. Intern. Med. 12, 436–439. Hillers, K.R., Dernell, W.S., Lafferty, M.H., Withrow, S.J. and Lana, S.E. 2005. Incidence and prognostic importance of lymph node metastases in dogs with appendicular osteosarcoma: 228 cases (1986–2003). J. Am. Vet. Med. Assoc. 226, 1364–1367. Kondo, Y., Matsunaga, S., Mochizuki, M., Kadosawa, T., Nakagawa, T., Nishimura, R. and Sasaki, N. 2008. Prognosis of canine patients with nasal tumors according to modified clinical stages based on computed tomography: a retrospective study. J. Vet. Med. Sci. 70, 207–212. Ladue, T.A., Dodge, R., Page, R.L., Price, G.S., Hauck, M.L. and Thrall, D.E. 1999. Factors influencing survival after radiotherapy of nasal tumors in 130 dogs. Vet. Radiol. Ultrasound. 40, 312–317. Lana, S.E., Dernell, W.S., Lafferty, M.H., Withrow, S.J. and LaRue, S.M. 2004. Use of radiation and a slow-release cisplatin formulation for treatment of canine nasal tumors. Vet. Radiol. Ultrasound. 45, 577–581. Lana, S.E., Dernell, W.S., LaRue, S.M., Lafferty, M.J., Douple, E.B., Brekke, J.H. and Withrow, S.J. 1997. Slow release cisplatin combined with radiation for the treatment of canine nasal tumors. Vet. Radiol. Ultrasound. 38, 474–478. Langova, V., Mutsaers, A.J., Phillips, B. and Straw, R. 2004. Treatment of eight dogs with nasal tumours with alternating doses of doxorubicin and carboplatin in conjunction with oral piroxicam. Aust. Vet. J. 82, 676–680. Lawrence, J.A., Forrest, L.J., Turek, M.M., Miller, P.E., Mackie, T.R., Jaradat, H.A., Vail, D.M., Dubielzig, R.R., Chappell, R. and Mehta, M.P. 2010. Proof of principle of ocular sparing in dogs with sinonasal tumors treated with intensity-modulated radiation therapy. Vet. Radiol. Ultrasound. 51, 561–570. Leeuwen, C.M., Oei, A.L., Crezee, J., Bel, A., Franken, N.A.P., Stalpers, L.J.A. and Kok, H.P. 2018. The alfa and beta of tumours: a review of parameters of the linear-quadratic model, derived from clinical radiotherapy studies. Radiat. Oncol. 13, 96. Malinowski, C. 2006. Canine and feline nasal neoplasia. Clin. Tech. Small Anim. Pract. 21, 89–94. Marlowe, K.W., Robat, C.S., Clarke, D.M., Taylor, A., Touret, M., Husbands, B.D. and Vail, D.M. 2018. Primary pulmonary histiocytic sarcoma in dogs: a retrospective analysis of 37 cases (2000–2015). Vet. Comp. Oncol. 16, 658–663. Maruo, T., Shida, T., Fukuyama, Y., Hosaka, S., Noda, M., Ito, T., Sugiyama, H., Ishikawa, T. and Madarame, H. 2011. Retrospective study of canine nasal tumor treated with hypofractionated radiotherapy. J. Vet. Med. Sci. 73, 193–197. Mason, S.L., Maddox, T.W., Lillis, S.M. and Blackwood, L. 2013. Late presentation of canine nasal tumours in a UK referral hospital and treatment outcomes. J. Small Anim. Pract. 54, 347–353. Morgan, M.J., Luriw, D.M. and Villamil, A.J. 2018. Evaluation of tumor volume reduction of nasal carcinomas versus sarcomas in dogs treated with definitive fractionated megavoltage radiation: 15 cases (2010–2016). BMC. Res. Notes. 11, 70. Northrup, N.C., Etue, S.M., Ruslander, D.M., Rassnick, K.M., Hutto, D.L., Bengtson, A., Rand, W. and Moore, A.S. 2001. Retrospective study of orthovoltage radiation therapy for nasal tumors in 42 dogs. J. Vet. Intern. Med. 15, 183–189. Pecceu, E., Serra Varela, J.C.S., Handel, I., Piccinelli, C., Milne, E. and Lawrence, J. 2020. Ultrasound is a poor predictor of early or overt liver or spleen metastasis in dogs with high-risk mast cell tumours. Vet. Comp. Oncol. 18, 389–401. Rassnick, K.M., Goldkamp, C.E., Erb, H.N., Scrivani, P.V., Njaa, B.L., Gieger, T.L., Turek, M.M., Mcniel, E.A., Proulx, D.R., Chun, R., Mauldin, G.E., Phillips, B.S. and Kristal, O. 2006. Evaluation of factors associated with survival in dogs with untreated nasal carcinomas: 139 cases (1993–2003). J. Am. Vet. Med. Assoc. 229, 401–406. Stevens, A., Turek, M., Vail, D., Christensen, N. and Forrest, L. 2020. Definitive-intent intensity modulated radiotherapy for modified-Adams’ stage 4 canine sinonasal cancer: a retrospective study of 29 cases (2011–2017). Vet. Radiol. Ultrasound. 61, 718–725. Turek, M., LaDue, T., Looper, J., Nagata, K., Shiomitsu, K., Keyerleber, M., Buchholz, J., Gieger, T. and Hetzel, S. 2020. Multimodality treatment including ONCEPT for canine oral melanoma: a retrospective analysis of 131 dogs. Vet. Radiol. Ultrasound. 61, 471–480. Yoshikawa, H., Lafferty, M.H., Griffin, L.R. and LaRue, S.H. 2023. A retrospective study of sinonasal tumors in 182 dogs treated with stereotactic radiotherapy (3×10Gy) (2010–2015). J. Vet. Intern. Med. 37, 2356–2367. | ||











| How to Cite this Article |
| Pubmed Style Mizuno R, Mori T. Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. Open Vet. J.. 2024; 14(7): 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 Web Style Mizuno R, Mori T. Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. https://www.openveterinaryjournal.com/?mno=184145 [Access: June 26, 2026]. doi:10.5455/OVJ.2024.v14.i7.3 AMA (American Medical Association) Style Mizuno R, Mori T. Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. Open Vet. J.. 2024; 14(7): 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 Vancouver/ICMJE Style Mizuno R, Mori T. Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. Open Vet. J.. (2024), [cited June 26, 2026]; 14(7): 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 Harvard Style Mizuno, R. & Mori, . T. (2024) Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. Open Vet. J., 14 (7), 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 Turabian Style Mizuno, Rui, and Takashi Mori. 2024. Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. Open Veterinary Journal, 14 (7), 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 Chicago Style Mizuno, Rui, and Takashi Mori. "Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases." Open Veterinary Journal 14 (2024), 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 MLA (The Modern Language Association) Style Mizuno, Rui, and Takashi Mori. "Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases." Open Veterinary Journal 14.7 (2024), 1538-1552. Print. doi:10.5455/OVJ.2024.v14.i7.3 APA (American Psychological Association) Style Mizuno, R. & Mori, . T. (2024) Prognostic factors and survival following radiation therapy for canine nasal tumors: A single-institution retrospective study of 166 cases. Open Veterinary Journal, 14 (7), 1538-1552. doi:10.5455/OVJ.2024.v14.i7.3 |

