




| Research Article | ||
Open Vet. J.. 2025; 15(7): 3308-3316 Open Veterinary Journal, (2025), Vol. 15(7): 3308-3316 Research Article Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trialGabriela Pereira Souza1, Lucas Wamser Fonseca Gonzaga1, Pablo Henrique Silva Avelar2, Jelieny Aparecida Claudino2, Marilda Onghero Taffarel3 and Marcos Ferrante1*1Department of Veterinary Medicine, Federal University of Lavras, Lavras, Brazil 2Department of Veterinary Medicine, University Center of Lavras, Lavras, Brazil 3Department of Veterinary Medicine, State University of Maringá, Umuarama, Brazil *Corresponding Author: Marcos Ferrante. UFLA - Department of Veterinary Medicine, Centro Administrativo - Aquenta Sol, Lavras, Brazil. Email: marcos.ferrante [at] ufla.br Submitted: 08/03/2025 Revised: 18/05/2025 Accepted: 11/06/2025 Published: 31/07/2025 © 2025 Open Veterinary Journal
ABSTRACTIntroduction: Presedation before general anesthesia helps reduce patient anxiety and facilitates anesthetic induction. Acepromazine and dexmedetomidine are widely used in dogs; however, these drugs cause cardiopulmonary alterations that may have a significant physiological impact when combined with the effects of propofol. Aim: This study aimed to evaluate the effect of premedication with acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol administered at a rate of 1 mg/kg/min to healthy dogs. Methods: Twenty-four healthy adult dogs were randomly divided into two groups according to the premedication protocol: ACP (0.02 mg/kg acepromazine associated with 0.3 mg/kg methadone) or DEX (2 µg/kg dexmedetomidine associated with 0.3 mg/kg methadone). In both groups, premedication was administered intramuscularly, and the dogs were subsequently administered propofol at a rate of 1 mg/kg/min using a syringe infusion pump. The sedation level, total propofol dose required for induction, induction time, and cardiopulmonary variables at baselin and pre-induction and postinduction periods were evaluated. Results: The DEX group showed a higher sedation score (p < 0.001), lower propofol requirement (p=0.005), shorter induction time (p=0.024), lower heart rate (HR) (p=0.036), lower respiratory rate (p=0.04), and higher incidence of post-induction hypercapnia (p < 0.001) compared to the ACP group. The incidence of myoclonus during anesthetic induction was higher in the ACP group (p=0.005). No animals exhibited apnea, desaturation, or hypotension. Conclusion: The use of 2 µg/kg dexmedetomidine and 0.3 mg/kg methadone as premedication promotes a higher degree of sedation, reducing the propofol dose and the incidence of myoclonus during anesthetic induction with propofol at a rate of 1 mg/kg/min. However, it had a greater impact on HR and respiratory parameters after induction compared with the combination of 0.02 mg/kg acepromazine and 0.3 mg/kg methadone. Keywords: Premedication, Anesthesia, Canine, Continuous infusion. IntroductionPre-sedation before anesthetic induction is recommended to aid in restraint, promote anxiolysis, facilitate induction, and reduce the amount of potentially more depressant drugs used in general anesthesia (Pereira and Lerche, 2024). Acepromazine and dexmedetomidine are among the main drugs used for pre-anesthetic sedation in dogs, and although used for the same purpose, they produce distinct effects (Bigby et al., 2017a; Martin-Flores et al., 2019). The combination of opioids in the protocol is frequently used to promote analgesia and enhance sedation, optimizing the use of lower doses of sedatives and tranquilizers (Monteiro et al., 2008). Ideal anesthetic induction includes smooth and rapid loss of consciousness with a low drug dose requirement, thereby minimizing cardiorespiratory adverse effects (Walters et al., 2022; Hamilton, 2024). Propofol is widely used as an anesthetic inducer in small animals because it promotes rapid and high-quality induction (Bigby et al., 2017a; Hamilton, 2024). However, significant adverse effects include hypotension, myocardial depression, respiratory depression, and post-induction apnea, which are associated with dose and administration rate (Bigby et al., 2017b; Walters et al., 2022; Hamilton, 2024). Additionally, myoclonic movements may occur during or after propofol administration, compromising induction quality (Hamilton, 2024). Propofol administration is performed by titration to achieve clinical effects, with various proposed dosing schemes that present wide variability (Sahinovic et al., 2018). Some authors have demonstrated that the dose and time required to achieve anesthetic induction are lower when using a reduced continuous infusion rate (Bigby et al., 2017b; Raillard et al., 2018; Walters et al., 2022). Considering the reduction in dose, induction time, and occurrence of post-induction apnea, Walters et al. (2022) concluded that the ideal infusion rate is 1 mg/kg/min in healthy dogs premedicated with dexmedetomidine and methadone. However, the authors did not evaluate the application and effects of this rate in another premedication protocol. Thus, the objective of the present study was to evaluate the effect of premedication with acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol administered at a rate of 1 mg/kg/min in healthy dogs. Our hypothesis was that dexmedetomidine would reduce the propofol dose and induction time but would increase the incidence of postinduction adverse effects. Materials and MethodsAnimalsThe study included adult dogs (classified by age according to body size, as per Cattai et al., 2019), nonbrachycephalic, with a body condition score between 4 and 6 (Laflamme, 1997), and categorized as American Society of Anesthesiologists score I based on the absence of abnormalities in pre-anesthetic evaluations (complete blood count, total protein and fractions, urea, creatinine, alanine aminotransferase, alkaline phosphatase, and electrocardiogram). The dogs underwent surgical procedures at the Veterinary Clinics Complex of the University Center of Lavras (UNILAVRAS) between December 2023 and March 2024.
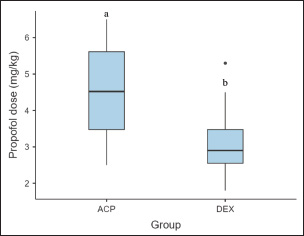
Fig. 1. Total dose of propofol for anesthetic induction in dogs that received premedication with 0.02 mg/kg acepromazine and 0.3 mg/kg methadone (ACP Group) or 2 µg/kg dexmedetomidine and 0.3 mg/kg methadone (DEX Group) (n=12). The boxes show the interquartile range, the whiskers show the minimum and maximum values, and the lines within the boxes represent the medians. Outliers are marked as points. Significance was set at p < 0.05. Different letters indicate statistical differences between groups. The exclusion criteria were conditions requiring alterations in the established protocols, such as allergic reactions to propofol, highly aggressive dogs requiring deeper sedation scores in premedication, continuous medication use (e.g., anxiolytics), complications necessitating additional therapy (e.g., severe bradycardia with hypotension before anesthetic induction), or cases where complete data collection was not possible. Study protocolDogs were randomly randomized into one of two groups using a random number generator (Excel 2016; Microsoft Corporation, WA, USA). The groups differed based on the type of premedication administered:
Anesthetic procedureIn a preparation room, all dogs received intramuscular premedication according to their assigned group: acepromazine (Acepran® 0.2%, Vetnil®) or dexmedetomidine (Dexdomitor® 0.5 mg/ml, Zoetis) combined with methadone (MYTedom® 10 mg/ml, Cristália®). The dogs were left undisturbed for 20 minutes. After this period, the sedation score was assessed using a previously published scale (Grint et al., 2009), ranging from 0 (no sedation) to 21 (deep sedation).
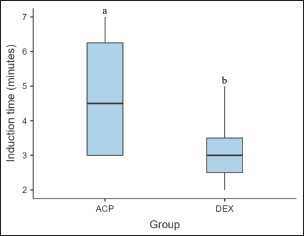
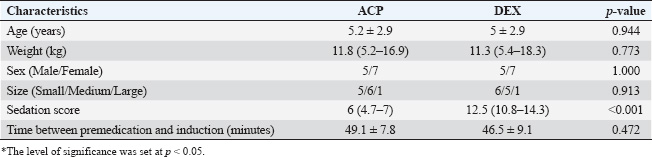
Fig. 2. Time (minutes) for anesthetic induction in dogs that received premedication with 0.02 mg/kg acepromazine and 0.3 mg/kg methadone (ACP Group) or 2 µg/kg dexmedetomidine and 0.3 mg/kg methadone (DEX Group) (n=12). The boxes show the interquartile range, the whiskers show the minimum and maximum values, and the lines within the boxes represent the medians. Outliers are marked as points. Significance was set at p < 0.05. Different letters indicate statistical differences between groups. Following sedation assessment, a peripheral catheter (Descarpack®, Brazil) with an appropriate gauge for the dog’s size was inserted and connected to an adapter plug (Foyomed®, Brazil) in the cephalic vein of the left thoracic limb. After venous access, the surgical site was clipped, and prophylactic antibiotic therapy with 30 mg/kg sodium cefalotin (Cefariston®; Blau Farmacêutica S.A.) was administered intravenously. The dogs were then transferred to the surgical center for anesthetic induction. Anesthetic induction was performed using a continuous infusion of propofol (Propovan® 10 mg/ml; Cristália) at a rate of 1 mg/kg/min via a syringe infusion pump (UniFusion SP50 Pro Vet, MedRena). An initial dose of 5 mg/kg of propofol was prepared in a 20-ml syringe connected to an extension line (Neonatal extension line 120 cm and 5 Fr; Embramed, Brazil), which was attached to a 30 × 0.8 mm hypodermic needle inserted directly into the adapter plug connected to the venous catheter. Induction and intubation were performed by the same experienced anesthetist in all cases. The start time of propofol administration was recorded to calculate the interval between premedication and anesthetic induction. The infusion of propofol was initiated, and the endpoint for stopping administration was determined by the presence of the following characteristics: loss of head support, ventromedial eye rotation, reduced or absent palpebral reflex, and low jaw and tongue tone. Once the anesthetic plane was confirmed, the infusion was stopped, the time was recorded, and the animals were intubated with an appropriately sized endotracheal tube. If intubation resistance was encountered, as demonstrated by a cough reflex, additional propofol would be administered, and the animal would be excluded from the study. Quantification of propofol dose and induction timeThe total propofol dose required for anesthetic induction was calculated by subtracting the residual volume in the syringe from the initial volume and converting the result to mg/kg. The volume in the extension line was disregarded because it was prefilled with propofol beyond the initial volume considered in the syringe. The total induction time was calculated based on the recorded start and end times of continuous infusion. Assessment of physiological variables and myoclonus occurrencePhysiological variables, including heart rate (HR), respiratory rate (RR), and systolic arterial pressure (SAP), were measured and recorded at three time points: before premedication (baseline), immediately before induction (pre-induction), and immediately after intubation (post-induction). During the postinduction period, oxygen saturation (SpO2) and end-tidal carbon dioxide (EtCO2) were also recorded. Two blinded observers recorded the physiological parameters, with one measuring HR and SAP and the other measuring RR, SpO2, and EtCO2. HR was measured via electrocardiographic monitoring using a multiparameter monitor (SDAMONITOR 12; SDAMed, Brazil). SAP was measured in the right thoracic limb using a vascular Doppler (DV 610V; Medmega®, Brazil) fixed in the palmar metacarpal region near the pad and a sphygmomanometer (SDA-ES1; SDAMed, Brazil) with a cuff size corresponding to approximately 40% of the midlimb diameter. Hypotension was defined as SAP 90 mm Hg. RR was determined by counting the respiratory movements for 60 seconds. Some dogs exhibited panting, making counting difficult. In such cases, a standard value of 160 breaths per minute was recorded for statistical purposes, following previous methodologies for panting dogs (Bigby et al., 2017b). Apnea was defined as the absence of respiratory movements for 30 seconds or more (Bigby et al., 2017a; Cattai et al., 2018). SpO2 was measured using a pulse oximeter placed on the tongue, while EtCO2 was recorded via sidestream capnography, with the highest value recorded within the first minute of the postinduction period. The oximeter and capnograph were integrated into the multiparameter monitor. Desaturation was defined as SpO2 below 90%, and hypercapnia was classified as EtCO2 greater than 45 mm Hg. If desaturation or EtCO2 exceeded 60 mm Hg during the monitoring period, manual ventilation was initiated and recorded. The same anesthetist responsible for anesthetic induction assessed the occurrence of myoclonus, which is characterized by involuntary muscle contractions, during propofol administration. The myoclonus score was recorded on a scale ranging from 0 (no contractions) to 3 (intense contractions) (Bell et al., 2011). Oxygen flow and additional anesthetic medications were initiated only after completing the collection of all postinduction parameters. Statistical analysisStatistical analyses were performed using JAMOVI software version 2.5.6. The significance level was set at p < 0.05. Data distribution was assessed using the Shapiro–Wilk test for numerical variables within groups. Data are summarized as mean ± SD for normally distributed variables or median (interquartile range) for nonparametric data. Numerical data between independent groups were compared using the Student’s t-test or Mann–Whitney test. Dependent physiological parameters (HR, RR, and SAP) were analyzed using repeated measures ANOVA or the Friedman test, followed by paired post hoc comparisons to evaluate differences between assessment time points. Ordinal qualitative variables (body condition score and sedation score) were assessed using the Mann–Whitney test, while nominal qualitative variables (size, sex, incidence of hypercapnia, desaturation, hypotension, and myoclonus) were analyzed using the Chi-square test. Table 1. Characteristics of the dogs included in the study, sedation score, and time between premedication and induction according to the group (ACP – premedication with 0.02 mg/kg acepromazine and 0.3 mg/kg methadone; DEX – premedication with 2 μg/kg dexmedetomidine and 0.3 mg/kg methadone) (n=12).
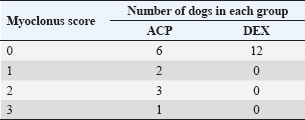
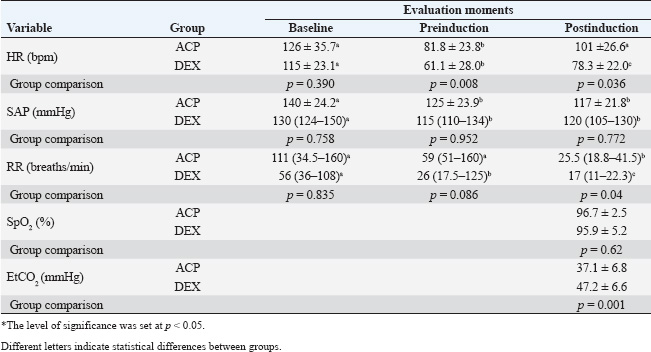
Ethical approvalInformed owner consent was obtained, and the study was approved by the Animal Ethics Committee (CEUA–UNILAVRAS). The research project registered under number 050/2023 was approved by the ethics committee for the use of animals at the Lavras University Center on 08/16/2023. ResultsA total of 24 dogs were included in the study, with 12 animals per group. The surgical procedures performed included orchiectomies (5), ovariohysterectomies (4), dental prophylaxis (7), simple nodulectomies (7), and third eyelid gland repositioning (1). There were no significant differences between the groups in age, weight, sex, size, or time between premedication and anesthetic induction. However, the sedation score was higher in the DEX group (Table 1). The dose of propofol (mg/kg) required for anesthetic induction was higher in the ACP group (4.6 ± 1.3) than in the DEX group (3.1 ± 1.0) (p=0.005) (Fig. 1). Additionally, the induction time (minutes) was longer in the ACP group (4.5 [3–6.25]) than in the DEX group (3 [2.5–3.5]) (p=0.024) (Fig. 2). During anesthetic induction, dogs in the ACP group had a higher incidence of myoclonus (6/12) than those in the DEX group (0/12) (p=0.005). The myoclonus score during anesthetic induction is presented in Table 2. The cardiovascular and respiratory physiological variables are presented in Table 3. In the ACP group, HR decreased between the baseline and pre-induction periods (p=0.008) and increased between the pre- and post-induction periods (p=0.011), with no differences in the final period compared with the baseline. In the DEX group, there was also a decrease in HR between the baseline and pre-induction periods (p < 0.001) and an increase between the pre- and post-induction periods (p=0.014). In the final period, however, HR remained lower than that at baseline (p=0.004). There was no difference between the groups in HR during the baseline period, but in the pre- and post-induction periods, animals in the DEX group had lower HR compared with the ACP group (p < 0.05). Table 2. Myoclonus score during anesthetic induction in dogs included in the study according to the group (ACP – premedication with 0.02 mg/kg acepromazine and 0.3 mg/kg methadone; DEX – premedication with 2 µg/kg dexmedetomidine and 0.3 mg/kg methadone) (n=12).
In both groups, there was a reduction in SAP between the baseline and preinduction periods (p < 0.05), with no difference between the pre- and postinduction periods. No hypotension was recorded at any evaluation time, and there were no differences between the groups. The ACP group showed a reduction in RR only between the pre- and post-induction periods (p=0.006), whereas in the DEX group, there was a progressive decrease in RR between all three time points (p < 0.01). In the postinduction period, the RR of the DEX group was lower than that of the ACP group (p=0.04). No animal experienced postinduction apnea. There was no difference between the groups in SpO2, and no animals experienced desaturation. However, the DEX group showed a higher EtCO2 after anesthetic induction compared with the ACP group (p=0.001), with a higher incidence of hypercapnia (p < 0.001) in the DEX group. DiscussionIn healthy dogs, premedication with dexmedetomidine or acepromazine at conservative doses in combination with methadone did not cause a significant cardiopulmonary impact during propofol induction at a rate of 1 mg/kg/min. Dexmedetomidine demonstrates a higher sedation potential, reduced propofol requirement, and provides a smoother induction; however, it also reduces the HR more and induces greater respiratory depression, which may be relevant in clinically unstable animals. Table 3. Cardiovascular and respiratory variables are presented as mean ± SD or median (interquartile range) measured at baseline, pre-induction, and post-induction, according to the group (ACP – premedication with 0.02 mg/kg acepromazine and 0.3 mg/kg methadone; DEX – premedication with 2 µg/kg dexmedetomidine and 0.3 mg/kg methadone) (n=12).
The goal of presedation before general anesthesia induction is to reduce stress, facilitate patient preparation, and facilitate transition to general anesthesia (Kramer et al., 2022). Moreover, sedative drugs reduce the requirement for propofol, which is beneficial in decreasing its dose-dependent adverse effects (Hamilton, 2024). However, it is important to consider that the drugs used for preanesthetic sedation also interfere with cardiopulmonary function (Kramer et al., 2022). Therefore, the choice of drugs and doses should be strategic to meet the premedication goals without increasing the physiological impact on the patient during anesthetic induction. In our study, we opted to use sedative drugs at doses commonly used in our routine, which are at the lower limit of the dose range recommended in the literature (Creighton and Lamont, 2024). The same doses of acepromazine, dexmedetomidine, and methadone have also been cited by other authors as standard in their hospital practice (Petruccione et al., (2021)). Despite the relatively low doses, the protocols were sufficient to allow the manipulation and performance of surgical preparation activities for all dogs without difficulty and proved to be applicable in clinical practice. The combination of opioids with sedatives helps intensify sedation, thereby enhancing the effect of the sedatives even at low doses (Monteiro et al., 2008; Bigby et al., 2017a; Kramer et al., 2022). Therefore, the effectiveness of the treatments is likely associated with concurrent use of methadone. It is important to note that no aggressive or difficult-to-handle animals were included in the study, as this could have led to different results and necessitated modifications to the sedation protocol. Our study showed that dogs in the DEX group had a higher degree of sedation and required a lower dose of propofol for anesthetic induction. This is an expected result since the sedative effects of dexmedetomidine are more pronounced than those of acepromazine (Bell et al., 2011), and the propofol requirement can be influenced by the degree of sedation (Hammond and England, 1994; Di Franco et al., 2023). However, some studies did not identify the same influence of premedication drugs on propofol dose (Bigby et al., 2017a; Kramer et al., 2022), although they performed anesthetic induction at a higher administration rate. Bigby et al. (2017a) induced dogs with propofol at a rate of 4 mg/kg/min, whereas Kramer et al. 2022 administered a bolus of 1 mg/kg every 10 seconds. It has been shown that the rate of propofol infusion influences the total induction dose (Bigby et al., 2017b; Walters et al., (2022)); thus, the infusion rate factor may override the sedative effect on the induction dose. This is an important observation to consider in studies evaluating factors influencing anesthetic induction, and standardizing propofol administration remains a challenge in veterinary medicine, limiting the comparison of results. Half of the dogs in the ACP group exhibited some degree of myoclonus during anesthetic induction, with two classified as mild, three as moderate, and one as severe, whereas none of the dogs in the DEX group showed any myoclonus. This is likely associated with the difference in sedation levels between the groups, as episodes of excitement during propofol administration may be exacerbated in less sedated animals (Davies, 1991). Petruccione et al. (2021) compared anesthetic induction in dogs premedicated with acepromazine or dexmedetomidine combined with methadone at the same doses used in our study, but used a propofol infusion rate of 2–4 mg/kg/min for induction and did not observe differences in the occurrence of myoclonus. Similarly, in the study by Bigby et al. (2017a), no difference in myoclonus was found in dogs premedicated with acepromazine (0.05 mg/kg) or dexmedetomidine (5 μg/kg) combined with methadone (0.5 mg/kg), with induction done with propofol at 4 mg/kg/min. Therefore, we believe that the slower rate of propofol administration used in our study may have contributed to the occurrence of myoclonus in the group with less sedation. The induction rate used was based on a study by Walters et al. (2022), who demonstrated less apnea time and a lower propofol requirement when administering the drug at 1 mg/kg/min, suggesting it to be an ideal rate for anesthetic induction in dogs. These authors used dexmedetomidine and methadone as premedication, so they did not demonstrate the effect of this rate in dogs with a lower degree of sedation, as was the case with the ACP group. Thus, it is important to consider that when using this infusion rate in dogs with lower sedation levels, myoclonus is likely to occur, which can range from mild to severe and may compromise the quality of anesthetic induction. We observed a reduction in HR in both groups at the preinduction moment, resulting from the effect of the preanesthetic medication used, with greater intensity in the DEX group. This result is expected because bradycardia is a common side effect of dexmedetomidine and may occur due to a reflex response to increased vascular resistance, combined with a central effect (Martin-Flores et al., 2019; Petruccione et al., 2021). After acepromazine administration, HR may remain unchanged or exhibit variable responses, with a mild increase in frequency often occurring reflexively due to a reduction in blood pressure (Monteiro et al., 2008; Creighton and Lamont, 2024). The result seen in the ACP group animals may be associated with the concurrent use of methadone, which increases vagal tone in dogs, resulting in reduced HR (Monteiro et al., 2008; Maiante et al., 2009). Dexmedetomidine and acepromazine have opposing mechanisms against vascular resistance (Petruccione et al., 2021); thus, it was expected that the DEX group would have a higher blood pressure than the ACP group. However, this difference was not observed. At the preinduction moment, when only the sedative effects of the drugs were predominant, both groups showed a slight reduction in arterial pressure, but still remained within physiological limits. This is likely associated with the use of conservative doses and the route of administration, as intramuscular injection avoids a rapid increase in the plasma concentration of the drugs. The effect of α2-agonists on arterial pressure is characterized by an initial elevation due to increased vascular resistance, followed by a reduction due to persistent bradycardia (Creighton and Lamont, 2024). According to Sinclair (2003), the intensity of the vasoconstrictor effect depends on the dose and route of administration, with lower doses being associated with predominantly central effects, without pronounced stimulation of peripheral adrenergic receptors. Moreover, the hypertensive peak is more common when the drug is administered intravenously. Similar to our results, other authors also did not show a significant increase in SAP in dogs premedicated with intramuscular dexmedetomidine at doses of 1 or 3 μg/kg (Pinelas et al., 2014). The reduction in arterial pressure resulting from acepromazine use is primarily mediated by α1-adrenergic receptor antagonism and is also dose-dependent (Creighton and Lamont, 2024). Monteiro et al. 2008 demonstrated that the use of a high dose of acepromazine (0.1 mg/kg) resulted in greater SAP reduction with incidences of hypotension compared with the combination of acepromazine (0.05 mg/kg) and methadone (0.5 mg/kg). The authors also observed that the combination of these drugs was more advantageous for sedation than the use of a higher dose of acepromazine alone. Rangel et al. 2020 also reported that doses greater than 0.025 mg/kg of acepromazine are not advantageous for sedation in dogs. Hypotension resulting from reduced vascular resistance, associated with a variable HR response, is the main hemodynamic effect reported after anesthetic induction with propofol (Hamilton, 2024). HR can be increased to maintain cardiac output when the baroreflex response is intact or reduced when this response is abolished (Mayer et al., 1993; Sato et al., 2005; Cattai et al., 2018). In both groups, we observed an increase in HR and maintenance of blood pressure after anesthetic induction, which suggests that the cardiac baroreflex was preserved during propofol administration at a rate of 1 mg/kg/min, compensating for any potential vasodilatory effect. It is likely that the infusion rate was responsible for maintaining the cardiovascular response. However, it is important to highlight that even at a dose of 2 μg/kg, dexmedetomidine induced a significant reduction in HR, keeping this parameter below baseline. This result should be considered because it may persist throughout the anesthetic maintenance period, potentially compromising cardiac output (Pinelas et al., 2014). Dogs that received dexmedetomidine showed a decrease in RR between the baseline and preinduction periods, which decreased further after anesthetic induction, maintaining a lower RR than the ACP group at this last moment. Additionally, the EtCO2 concentration after induction was higher in dogs that received dexmedetomidine. Nine dogs in the DEX group (75%) had an EtCO2 > 45 mmHg (ranging from 46 to 56 mmHg), and only one dog in the ACP group (8%) had an EtCO2=47 mmHg. Increased arterial CO2 pressure can occur after the administration of anesthetics like propofol, while α2-adrenergic agonists may interfere with the neuro-respiratory response to this increase, in addition to reducing the RR (Lerche and Muir, 2004). On the other hand, acepromazine may reduce the RR but does not cause significant changes in blood gases as tidal volume is increased, maintaining stable respiratory function (Bigby et al., 2017a; Rangel et al., 2020; Creighton and Lamont, 2024). Respiratory depression after anesthetic induction is a dose-dependent effect commonly described after the use of propofol (Hamilton, 2024). In this study, we found that dexmedetomidine was associated with postinduction hypoventilation, even though it reduced the propofol requirement, contributing a negative effect on respiratory function. Opioids also have a depressive effect on the respiratory system by acting at different supraspinal sites, which can lead to increased CO2 pressure (Simon and Lizarraga, 2024). The combination of an α2-agonist with an opioid may intensify this effect (Sinclair, 2003; Pinelas et al., 2014). Thus, we emphasize the importance of strict monitoring of respiratory parameters in dogs receiving dexmedetomidine combined with an opioid, even at low doses. Moreover, caution should be exercised when using this protocol in animals with preexisting ventilatory impairment. This study has some limitations. More reliable cardiopulmonary measures, such as invasive blood pressure and blood gas analysis, were not performed, which could have provided more relevant information. However, since this was a clinical study conducted with healthy routine dogs, the instrumentation and the cost of obtaining these measurements were not justifiable. Additionally, the dogs were not acclimatized, which resulted in the baseline data reflecting stress-related changes, which is common in a real-world situation. Despite this, we believe that the study results are useful for guiding clinical practice, demonstrating the effects of drugs commonly used in routine care, and providing guidance on what to expect from drug combinations at the doses used. ConclusionThe use of 2 μg/kg dexmedetomidine combined with 0.3 mg/kg methadone as premedication resulted in a higher degree of sedation, reducing the propofol dose and the incidence of myoclonus during anesthetic induction with propofol at a rate of 1 mg/kg/min. However, it also had a greater impact on HR and respiratory parameters after induction when compared with the combination of 0.02 mg/kg acepromazine and 0.3 mg/kg methadone. AcknowledgmentsThe authors thank the Federal University of Lavras, the Veterinary Clinic Complex of the Lavras University Center, and the Coordination for the Improvement of Higher Education Personnel. Conflict of interestThe authors declare no conflict of interest. FundingThis research did not receive any specific funding. Authors’ contributionsG.P.S.: conceptualization, data collection and curation, formal analysis, methodology, writing-original draft; L.W.F.G.: Conceptualization, data curation, formal analysis; P.H.S.A.: Data collection and curation; J.A.C.: Data collection and curation; M.O.T.: conceptualization, methodology, writing-review and editing; M.F.: conceptualization, methodology, writing-review and editing, supervision, project administration. Data availabilityThe data presented in this study are available upon request from the corresponding author. ReferencesBell, A.M., Auckburally, A., Pawson, P., Scott, E.M. and Flaherty, D. 2011. Two doses of dexmedetomidine in combination with buprenorphine for premedication in dogs: a comparison with acepromazine and buprenorphine. Vet. Anaesth. Analg. 38, 15–23; doi:10.1111/j.1467-2995.2010.00576.x. Bigby, S.E., Beths, T., Bauquier, S. and Carter, J.E. 2017a. Post-induction apnoea in dogs premedicated with acepromazine or dexmedetomidine and anaesthetised with alfaxalone or propofol. Vet. Anaesth. Analg. 44, 1007–1015; doi:10.1016/j.vaa.2016.10.004. Bigby, S.E., Beths, T., Bauquier, S. and Carter, J.E. 2017b. Effect of rate of administration of propofol or alfaxalone on induction dose requirements and occurrence of apnea in dogs. Vet. Anaesth. Analg. 44, 1267–1275; doi:10.1016/j.vaa.2017.03.005. Cattai, A., Bizzotto, R., Cagnardi, P., Di Cesare, F. and Franci, P. 2019. A pharmacokinetic model optimized by covariates for propofol target-controlled infusion in dogs. Vet. Anaesth. Analg. 46, 568–578; doi:10.1016/j.vaa.2019.04.009. Cattai, A., Rabozzi, R., Ferasin, H., Isola, M. and Franci, P. 2018. Haemodynamic changes during propofol induction in dogs: new findings and approach of monitoring. BMC Vet. Res. 14:282; doi:10.1186/s12917-018-1608-8. Creighton C.M. and Lamont L.A. 2024. Sedatives and tranquilizers. In veterinary anesthesia and analgesia: the sixth edition of Lumb and Jones, 6th edn. Eds. Lamont, L., Grimm, K., Robertson, S., Love, L. and Schroeder, C. Charlottetown, Prince Edward Island, Canada: John Wiley & Sons, pp: 333–354. Davies, C. 1991. Excitatory phenomena following the use of propofol in dogs. Vet. Anaesth. Analg. 18(1), 48–51; doi:10.1111/j.1467-2995.1991.tb00014.x. Di Franco, C., Evangelista, F. and Briganti, A. 2023. Multiple uses of dexmedetomidine in small animals: a mini review. Front. Vet. Sci. 10, 1135124; doi:10.3389/fvets.2023.1135124. Grint, N.J., Burford, J. and Dugdale, A.H. 2009. Does pethidine affect the cardiovascular and sedative effects of dexmedetomidine in dogs? J. Small Anim. Pract. 50, 62–66; doi:10.1111/j.1748-5827.2008.00670.x. Hamilton, S.M. 2024. Injectable anesthetics. In Veterinary anesthesia and analgesia: the sixth edition of Lumb and Jones, 6th edn). Eds. Lamont, L., Grimm, K., Robertson, S., Love, L. and Schroeder, C. John Wiley & Sons; pp: 462–481. Hammond, R.A. and England, G.C.W. 1994. The effect of medetomidine premedication upon propofol induction and infusion anaesthesia in the dog. Vet. Anaesth. Analg. 21(1), 24–28; doi:10.1111/j.1467-2995.1994.tb00478.x. Kramer, B.M., Hector, R.C., Rezende, M.L., Hess, A.M. and Mama, K.R. 2022. Sedative and cardiopulmonary effects of intramuscular combinations of hydromorphone, acepromazine, dexmedetomidine, and glycopyrrolate followed by intravenous propofol and inhalant isoflurane anestesia in healthy dogs. Am. J. Vet. Res. 83(10), ajvr.22.06.0098; doi:10.2460/ajvr.22.06.0098. Laflamme, D. 1997. Developmental and validation of a body condition score system for dogs. Canine Practice 22(4), 10–15. Lerche, P. and Muir, W.W. 2004. Effect of medetomidine on breathing and inspiratory neuromuscular drive in conscious dogs. Am. J. Vet. Res. 65, 720–724; doi:10.2460/ajvr.2004.65.720. Maiante, A.A., Teixeira-Neto, F.J., Beier, S.L., Corrente, J.E. and Pedroso, C.E.B.P. 2009. Comparison of the cardio-respiratory effects of methadone and morphine in conscious dogs. J. Vet. Pharmacol. Ther. 32(4), 317–328; doi:10.1111/j.1365-2885.2008.01042.x. Martin-Flores, M., Mostowy, M.M., Pittman, E., Sakai, D.M., Mohammed, H.O., Gleed, R.D. and Campoy, L. 2019. Investigation of associations between preoperative acepromazine or dexmedetomidine administration and development of arterial hypotension or bradycardia in dogs undergoing ovariohysterectomy. J. Am. Vet. Med. Assoc. 255(2), 193–199; doi:10.2460/javma.255.2.193. Mayer, N., Legat, K., Weinstabl, C. and Zimpfer, M. 1993. Effects of propofol on the function of normal, collateral-dependent, and ischemic myocardium. Anesth. Analg. 76(1), 33–39; doi:10.1213/00000539-199301000-00006. Monteiro, E.R., Rodrigues Junior, A., Assis, H.M.Q., Campagnol, D. and Quitzan, J.G. 2009. Comparative study on the sedative effects of morphine, methadone, butorphanol or tramadol, in combination with acepromazine, in dogs. Vet. Anaesth. Analg. 36, 25–33; doi:10.1111/j.1467-2995.2008.00424.x. Pereira, C.H.R. and Lerche, P. 2024. Dogs and cats. In Veterinary anesthesia and analgesia: the sixth edition of Lumb and Jones, 6th edn. Eds. Lamont, L., Grimm, K., Robertson, S., Love, L. and Schroeder, C. Columbus, OH: John Wiley & Sons, pp: 1157–1165. Petruccione, I., Murison, P. J., Flaherty, D. and Auckburally, A. 2021. Comparison between dexmedetomidine and acepromazine in combination with methadone for premedication in brachycephalic dogs undergoing surgery for brachycephalic obstructive airway syndrome. Vet. Anaesth. Analg. 48, 305–313; doi:10.1016/j.vaa.2020.09.008. Pinelas, R., Alibhai, H.I.K., Mathis, A., Lozano, A.J. and Brodbelt, D.C. 2014. Effects of different doses of dexmedetomidine on anaesthetic induction with alfaxalone – a clinical trial. Vet. Anaesth. Analg. 41, 378–385; doi:10.1111/vaa.12121. Raillard, M., Love, E.J. and Murison, P.J. 2018. Effect of predosing versus slow administration of propofol on the dose required for anaesthetic induction and on physiologic variables in healthy dogs. Vet. Anaesth. Analg. 45(4), 414–422; doi:10.1016/j.vaa.2018.02.004. Rangel, J.P.P., Monteiro, E.R., Bitti, F.S., Junior, J.S.N. and Campagnol, D. 2020. Hemodynamic, respiratory and sedative effects of progressively increasing doses of acepromazine in conscious dogs. Vet. Anaesth. Analg. 47(4), 447–453; doi:10.1016/j.vaa.2020.02.007. Sahinovic, M.M., Struys, M.M.R.F. and Absalom, A.R. 2018. Clinical pharmacokinetics and pharmacodynamics of propofol. Clin. Pharmacokinet. 57, 1539–1558; doi:10.1007/s40262-018-0672-3. Sato, M., Tanaka, M., Umehara, S. and Nishikawa, T. 2005. Baroreflex control of heart rate during and after propofol infusion in humans. Br. J. Anaesth. 94(5), 577–581; doi:10.1093/bja/aei092. Simon, B.T. and Lizarraga, I. 2024. Opioids. In Veterinary anesthesia and analgesia: the sixth edition of Lumb and Jones, 6th edn. Eds. Lamont, L., Grimm, K., Robertson, S., Love, L. and Schroeder, C. John Wiley & Sons, pp: 355–397. Sinclair, M.D. 2003. A review of the physiological effects of a2-agonists related to the clinical use of medetomidine in small animal practice. Can. Vet. J. 44(11), 885–897. Walters, K., Lehnus, K., Liu, N-C. and Bigby, S.E. 2022. Determining an optimum propofol infusion rate for induction of anaesthesia in healthy dogs: a randomized clinical trial. Vet. Anaesth. Analg. 49, 243–250; doi:10.1016/j.vaa.2021.07.006. | ||
| How to Cite this Article |
| Pubmed Style Souza GP, Gonzaga LWF, Avelar PHS, Claudino JA, Taffarel MO, Ferrante M. Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. Open Vet. J.. 2025; 15(7): 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 Web Style Souza GP, Gonzaga LWF, Avelar PHS, Claudino JA, Taffarel MO, Ferrante M. Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. https://www.openveterinaryjournal.com/?mno=246483 [Access: June 27, 2026]. doi:10.5455/OVJ.2025.v15.i7.42 AMA (American Medical Association) Style Souza GP, Gonzaga LWF, Avelar PHS, Claudino JA, Taffarel MO, Ferrante M. Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. Open Vet. J.. 2025; 15(7): 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 Vancouver/ICMJE Style Souza GP, Gonzaga LWF, Avelar PHS, Claudino JA, Taffarel MO, Ferrante M. Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. Open Vet. J.. (2025), [cited June 27, 2026]; 15(7): 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 Harvard Style Souza, G. P., Gonzaga, . L. W. F., Avelar, . P. H. S., Claudino, . J. A., Taffarel, . M. O. & Ferrante, . M. (2025) Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. Open Vet. J., 15 (7), 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 Turabian Style Souza, Gabriela Pereira, Lucas Wamser Fonseca Gonzaga, Pablo Henrique Silva Avelar, Jelieny Aparecida Claudino, Marilda Onghero Taffarel, and Marcos Ferrante. 2025. Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. Open Veterinary Journal, 15 (7), 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 Chicago Style Souza, Gabriela Pereira, Lucas Wamser Fonseca Gonzaga, Pablo Henrique Silva Avelar, Jelieny Aparecida Claudino, Marilda Onghero Taffarel, and Marcos Ferrante. "Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial." Open Veterinary Journal 15 (2025), 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 MLA (The Modern Language Association) Style Souza, Gabriela Pereira, Lucas Wamser Fonseca Gonzaga, Pablo Henrique Silva Avelar, Jelieny Aparecida Claudino, Marilda Onghero Taffarel, and Marcos Ferrante. "Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial." Open Veterinary Journal 15.7 (2025), 3308-3316. Print. doi:10.5455/OVJ.2025.v15.i7.42 APA (American Psychological Association) Style Souza, G. P., Gonzaga, . L. W. F., Avelar, . P. H. S., Claudino, . J. A., Taffarel, . M. O. & Ferrante, . M. (2025) Effect of acepromazine or dexmedetomidine associated with methadone on anesthetic induction with propofol at a rate of 1 mg/kg/min in healthy dogs: A randomized clinical trial. Open Veterinary Journal, 15 (7), 3308-3316. doi:10.5455/OVJ.2025.v15.i7.42 |

