




| Case Report | ||
Open Vet. J.. 2025; 15(6): 2909-2914 Open Veterinary Journal, (2025), Vol. 15(6): 2909-2914 Case Report Video otoscopy-assisted Holmium: yttrium-aluminum- garnet laser excision of aural masses in four dogsAdheip Prabakaran1*, Julia P. Sumner2 and Sophie A. Tyler21Small Animal Specialist Hospital, Tuggerah, Australia 2Small Animal Specialist Hospital, North Ryde, Australia *Corresponding Author: Adheip Prabakaran. Small Animal Specialist Hospital, Tuggerah, Australia. Email: aprabakaran [at] sashvets.com Submitted: 18/03/2025 Revised: 08/05/2025 Accepted: 13/05/2025 Published: 30/06/2025 © 2025 Open Veterinary Journal
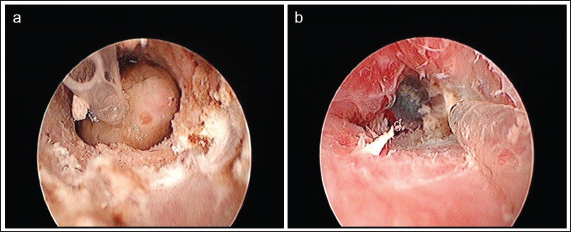
AbstractBackground: This case series reports the outcomes of four dogs that underwent video otoscopy-assisted laser excision (VALE) of aural masses using a Holmium: yttrium-aluminum-garnet (Ho:YAG) laser. Case Description: All cases underwent excision of aural masses by snare polypectomy and laser ablation of the stalk or direct excision of the mass with a Ho:YAG laser. The first three cases underwent VALE and were free of clinical signs at follow-up times ranging from 197 to 403 days post procedure. In one case, the direct application of the laser on the mass resulted in thermal necrosis of the submitted tissue and an open histopathological diagnosis. In the fourth case, VALE was unsuccessful due to an intimate adhesion of the mass with the tympanic bulla. This patient underwent total ear canal ablation and lateral bulla osteotomy (TECALBO), which subsequently developed a deep surgical site infection and was revised. The patient experienced complete recovery at 232 days post TECALBO. Conclusion: VALE of aural masses using a Ho:YAG laser is a minimally invasive and effective treatment for aural masses in dogs in the medium term, providing an alternative to TECALBO in three out of four of our cases. Direct excision of the mass using a laser can cause thermal necrosis of the tissue, making histopathologic diagnosis more challenging. More studies are required to determine the contraindications of this technique and to better quantify the outcomes and complications. Keywords: Aural masses, Dogs, Laser, Minimally invasive surgery, Otitis externa. IntroductionAural masses are an uncommon primary cause of otitis externa in dogs. Such cases are often refractory to medical management alone and are usually treated by excision of the ear canal by total ear canal ablation with concurrent lateral bulla osteotomy (TECALBO). This procedure is invasive and painful. Additionally, postoperative complications associated with TECALBO have a reported incidence of 21%–82% (Smeak, 2011). These complications include facial or hypoglossal nerve injury, Horner’s syndrome, incisional dehiscence, seroma, and superficial and deep wound infection (Mason et al., 1988; Beckman et al., 1990; Smeak, 2011; Spivack et al., 2013; Coleman and Smeak, 2016). Alternative treatment options have been investigated to mitigate morbidity associated with TECALBO. An alternative, less-invasive technique is traction avulsion. This procedure does not require specialized equipment or training; however, it is associated with high recurrence rates. In one report, inflammatory polyps that were removed by simple traction avulsion reoccurred in 57% of cats (Greci et al., 2014). In another report, there was clinical resolution in four out of six dogs that underwent traction-avulsion for aural inflammatory polyps (Schuldenfrei et al., 2023). It has, therefore, been proposed that laser ablation of the stalk may reduce this reoccurrence rate (Greci and Mortellaro, 2016). There are several promising reports describing the use and outcome of video-assisted laser excision (VALE) of aural masses in veterinary patients. One study demonstrated a lower reoccurrence rate of ceruminous aural tumors after CO2 laser ablation than that reported with traction avulsion alone (Pieper et al., 2023). To date, there have been no studies reporting the outcome of treating such masses with a Holmium: yttrium-aluminum-garnet (Ho:YAG) laser. Here, we report the use, complications, and outcomes of Ho:YAG laser for the excision of aural masses in four dogs. Case 1A 16.5 kg, 13-year-old male neutered cocker spaniel was referred to our specialist referral hospital for a right- sided aural mass. Conscious otoscopic examination using a handheld otoscope revealed a round, well- circumscribed, smooth mass at the entrance of the right horizontal ear canal. Ear cytology revealed occasional Articles published in Open Veterinary Journal are licensed under a Creative Commons Attribution-NonCommercial 4.0 International License rod-shaped bacteria, moderate numbers of degenerate neutrophils in the right ear, and moderate numbers of Malassezia in the left ear. Initial treatment consisted of enrofloxacin 1.5% (Baytril, Elanco Animal Health) and dexamethasone acetate 0.05% in hypromellose 5 mg/ml (Methopt, Viatris), 0.7 ml, topically in the right ear, q 12 hours), miconazole nitrate, polymyxin B, prednisolone acetate (Surolan, Elanco Animal Health), 0.5 ml, topically in the left ear, q 12 hours) and twice weekly cleaning of the right ear with 2.0 g/l poly(hexamethylene) biguanidine hydrochloride 1.2 g/l disodium edetate (Otoflush® Dermcare). After 7 days of topical treatment, the patient was anesthetized, and computed tomography (CT) of the head was performed. The findings revealed a pedunculated right external ear canal mass with secondary tympanic bulla fluid accumulation. There was no evidence of otitis interna. A right-sided great auricular bupivacaine (0.6 mg/kg) nerve block was performed and the right ear mass was removed under video otoscopy using a polypectomy snare. There was marked hemorrhage post removal obscuring visualization of the tympanic membrane preventing adequate visualization for flushing of the middle ear. Small polypoid masses in the left ear canal were noted but no action was taken. The right ear mass was submitted for histopathology and the patient was discharged on the day of the procedure with prednisolone (0.55 mg/kg PO q 24 hours), paracetamol (14 mg/kg PO q 8 hours), enrofloxacin 1.5%, and dexamethasone acetate 0.05% in hypromellose 0.5% (0.7 ml topically in the right ear, q 12 hours). Histopathology revealed a cutaneous extramedullary plasmacytoma with tumor cells extending to the margins of the mass. On post-procedure examination, there was no cytological evidence of microbial overgrowth of the right external ear canal; however, a remnant of the mass was visible on hand-held otoscopy after 10 days. Otoscopic examination after 20 days revealed that the mass had enlarged and occluded the external ear canal. Due to reoccurrence of the mass revision surgery was recommended by either VALE or TECALBO. The owner of the patient chose laser excision because it was a less invasive option. The patient was anesthetized and a Ho:YAG laser (Lisa Sphinx Jr Holmium Laser, Agiliti Health) was used to excise the right aural mass using 0.8 J and 8 Hz under video guidance. A smaller portion of the mass was found more proximally within the ear canal and ablated. The external ear canal was lavaged copiously with warmed sterile saline allowing visual verification of complete excision. The tympanic membrane was intact and a myringotomy was performed. Brown keratinous debris was suctioned from the middle ear. Cytology of the right external ear canal revealed occasional rod-shaped bacteria. The patient was discharged on the day of the procedure with prednisolone (0.55 mg/kg PO q 24 hours), paracetamol (14 mg/kg PO q 8 hours), marbofloxacin (Zeniquin, Zoetis) (2.77 mg/kg PO q 24 hours), and a suspension of enrofloxacin 1.5%, ketoconazole 2%, and dexamethasone acetate 0.05% in hypromellose 0.5% (0.7 ml topically in the right ear, q 12 hours). The patient represented for assessments at 7, 14, and 28 days post VALE. Conscious otoscopy at each revisit revealed no gross evidence of the mass or cytological evidence of microbial overgrowth. Topical antimicrobials were continued for 4 weeks and oral marbofloxacin for 7 weeks post Ho:YAG excision of the mass. The referring veterinarian performed further follow-up examinations. The last known examination with the referring veterinarian revealed no abnormalities on otoscopic examination 403 days after laser excision of the aural mass. The patient was euthanized due to an unrelated orthopedic disease 16 months post procedure. Case 2A 7.3 kg, 13-year-old female spayed Chihuahua cross was referred for assessment of a mass in the left horizontal ear canal. The referring veterinarian performed a CT scan of the head, chest, and abdomen, which demonstrated a discrete mass in the left horizontal ear canal with no evidence of metastatic disease or middle ear pathology. The referring veterinarian recommended TECALBO, but the owner declined and chose a less invasive procedure, prompting referral. On conscious otoscopic examination a white, bulbous mass was detected in the left horizontal ear canal with dark ceruminous exudate throughout the ear canal. The right ear canal was unremarkable. Left ear cerumen cytology revealed large numbers of degenerate neutrophils with moderate numbers of coccoid- shaped and filamentous bacteria. Initial treatment with enrofloxacin 1.5% and dexamethasone acetate 0.05% in hypromellose 0.5% (0.5 ml, topically in the left ear q 12 hours) and twice weekly ear cleaning with 2.0 g/l polyhexamethylene biguanidine hydrochloride 1.2 g/l disodium edetate was commenced. After 7 days of medical treatment for otitis externa the patient presented for excision of the mass. The patient was anaesthetised and a left great auricular bupivacaine (1 mg/kg) nerve block was performed prior to video otoscopy. The left ear canal was copiously lavaged with sterile saline using a 4G rigid catheter inserted through the videoscope portal. The mass was noted to be close to the tympanic membrane and could not be removed using a polypectomy snare (Fig. 1a). The Ho:YAG laser was used to directly excise the mass by ablating the tissue at its base. The mass was removed in two parts. A tear in the tympanic membrane was visualized after mass excision and was suspected to be iatrogenic. Following excision the site was inspected for complete excision (Fig. 1b). The patient did not develop any immediate clinical signs associated with the iatrogenic tear of the tympanic membrane and was discharged on the day of the procedure with prednisolone (0.7 mg/kg PO q 24 hours), paracetamol (12 mg/kg PO q 8 hours), topical enrofloxacin 1.5%, and dexamethasone acetate 0.05% in hypromellose 0.5% (0.5 ml, topically in the left ear, q 12 hours). Histopathological examination revealed extensive coagulation necrosis of the submitted tissue. Due to thermal artifacts associated with the use of the laser, a histopathological diagnosis could not be reached.
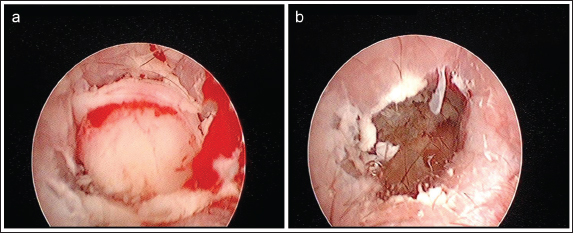
Fig. 1. Video otoscopic images of case 2 showing the gross appearance of the mass before (a) and after (b) laser excision. Post-procedure examinations were performed after 7, 14, and 40 days. The owner did not note any sign of aural discomfort post procedure. During all postoperative examinations, conscious hand-held otoscopy was performed revealing no evidence of mass reoccurrence. On otoscopic examination, 7 days post procedure minimal erythema of the left ear canal was noted. The last known examination of the patient was 331 days post procedure during a routine examination by the referring veterinarian. Both ears were grossly normal on otoscopic examination and excessive aural exudate was not noted. Case 3A 12.6 kg, 8.9-year-old male neutered Pug cross presented for recurrent, right unilateral otitis externa. Ten days prior to referral a mass was noted along the right ear canal. Conscious otoscopic examination revealed a brown moist exudate with an erythematous mass occluding the horizontal ear canal. A CT scan revealed complete filling of the right tympanic bulla with soft-tissue-attenuating material, which did not significantly enhance contrast. Mild thickening of the bulla wall ventrally with multiple ovoid regions of lysis was observed in the bulla wall. Due to bulla wall involvement, TECALBO surgery was discussed but Ho:YAG laser excision was recommended in the first instance for middle ear sampling and lavage. Cytology revealed large numbers of coccoid-shaped bacteria, moderate numbers of degenerate neutrophils, and small numbers of rod-shaped bacteria. Initial treatment consisted of enrofloxacin 1.5% and dexamethasone acetate 0.05% in hypromellose 0.5% (0.7 ml topically in the right ear, q 12 hours). After 7 days of topical antimicrobial treatment, the patient presented for excision of the mass. After the patient was anesthetized and copious lavage of the right external auditory canal was performed, the mass was found to be completely occluding the horizontal ear canal (Fig. 2a). A polypectomy snare was used to remove the mass. The stalk of the mass was then ablated using a Ho:YAG laser. The site was inspected following excision revealing complete mass excision (Fig. 2b). The tympanic membrane was found to be ruptured; however, this was not deemed to be iatrogenic. A large quantity of white keratinous debris was lavaged from the right middle ear. Cytology of the right middle ear revealed large numbers of squames with few coccoid-shaped bacteria in some high- power fields. Following the procedure the patient was discharged with paracetamol (9.9 mg/kg PO q 12 hours), amoxycillin clavulanate (23.8 mg/kg PO q 12 hours), prednisolone (0.6 mg/kg PO q 24 hours), and topical enrofloxacin 1.5% and dexamethasone acetate 0.05% in hypromellose 0.5% (0.7 ml, topically in the right ear, q 12 hours). Histopathology of the mass revealed a fibroepithelial polyp. Culture and susceptibility of the right middle ear sample to Staphylococcus pseudintermedius sensitive to amoxycillin clavulanate. Post-procedure examinations were performed after 8, 27, 50, and 197 days. The patient was reported to have minimal aural pruritus and had a grossly clean right external auditory canal without regrowth of the mass on hand-held otoscopy at all post-procedure examinations. On day 27 topical antimicrobial therapy was discontinued and replaced with a 1:1 solution of dexamethasone acetate 0.05% in hypromellose 0.5% (0.5 ml topically in the right ear, twice weekly). The ear was free of microbial overgrowth at all reexaminations. Case 4A 23 kg, 9.2-year-old castrated male British bulldog presented with recurrent, left unilateral otitis externa. The patient had a long history of chronic bilateral aural irritation. The left ear had been more severely affected in the 12 months prior to referral. Conscious hand-held otoscopic examination revealed a moderate to large volume of brown, mucoid discharge in the left ear canal obscuring visualization of the tympanic membrane. There was scant ceruminous discharge in the right ear. Cytology of the left ear cerumen revealed numerous neutrophils and coccoid-shaped bacteria. Based on these findings enrofloxacin 1.5% and dexamethasone acetate 0.05% in hypromellose 0.5% were commenced (0.6 ml topically in the left ear, q 12 hours). A reexamination 3 weeks later revealed ongoing aural irritation; therefore, a CT scan and video otoscopy were performed.
Fig. 2. Video otoscopic images of case 3 showing the gross appearance of the mass before (a) and after (b) laser excision. The patient was anesthetized, and a CT scan of the head and neck was performed, which revealed bilateral chronic otitis externa with irregular thickening of the left tympanic bulla with multifocal, small, punctate areas of osteolysis containing a large amount of non- contrast enhancing soft tissue attenuating material. The left horizontal ear canal contained a large quantity of non-contrast enhancing soft-tissue attenuating material. Video endoscopic examination revealed an aural mass following copious lavage of the aural discharge. The mass was biopsied using biopsy forceps through the video endoscope port but it was not possible to remove the mass in its entirety. Following the procedure the patient was discharged with paracetamol (10.8 mg/ kg PO q 12 hours), topical enrofloxacin 1.5%, and dexamethasone acetate 0.05% in hypromellose 0.5% (0.6 ml topically in the left ear, q 12 hours). A histopathologic diagnosis of fibroepithelial polyp was obtained and VALE of the left aural polyp was recommended. The patient was anesthetized, and following initial lavage, the mass was observed completely obstructing the horizontal ear canal close to the tympanic membrane. The Ho:YAG laser was used to ablate the attachments of the mass within the proximal external ear canal but the mass was embedded within the tympanic bulla and could not be removed via video otoscopy. Laser excision was, therefore, abandoned. The patient was discharged the following day with oral paracetamol (10.8 mg/kg PO q 12 hours), enrofloxacin 1.5%, and dexamethasone acetate 0.05% in hypromellose 0.5% (0.6 ml, topically in the left ear, q 12 hours). Due to the inability to excise the mass via video endoscopic laser ablation, a TECALBO was recommended and performed 33 days after attempted laser ablation. Histopathologic diagnosis of the middle ear following submission of the excised ear canal was consistent with tympanokeratoma (cholesteatoma). The patient represented 10 days after TECALBO surgery with purulent discharge from the surgical site. The surrounding skin was cleaned with chlorhexidine solution and the open wound was flushed with sterile saline. Bacterial culture and susceptibility testing of deep tissue revealed moderate growth of multidrug-resistant Pseudomonas aeruginosa. The patient represented 15 days after TECALBO surgery, and dehiscence of the proximal half of the surgical site was noted. CT of the head was repeated revealing thickening of the soft tissue consistent with regional cellulitis and inflammation. No large abscesses were detected. Under general anesthesia, the surgical site was sharply debrided and lavaged copiously with sterile saline. A collagen gentamicin implant (Collatamp®G, SERB Pharmaceuticals) was placed prior to closure. The patient remained hospitalized for 5 days following surgery receiving gentamicin intravenously (10 mg/kg IV q 24 hours) before discharge. The patient presented for postoperative examination 12 days after the revision of TECALBO. The surgical wound was intact and there was no discharge or discomfort during palpation. The last known examination 232 days after the initial TECALBO surgery showed full recovery and healing of the surgical site. DiscussionThis case series reports good medium-term outcomes in three out of four dogs who underwent VALE. In these three cases, the procedure was performed minimally invasively and the patients were discharged the same day of the procedure. The only intraoperative complication encountered was iatrogenic damage to the tympanic membrane in one case which did not cause any adverse clinical signs. A histopathological diagnosis could not be obtained for another case due to thermal necrosis of the submitted tissue. This severely limits our ability to predict prognosis and tailor adjunctive medical treatments. The authors, therefore, caution against the direct application of the Ho:YAG laser on tissue without first obtaining samples for histopathology. No postoperative complications directly associated with the procedure were reported. In the fourth case, laser excision of the mass was unsuccessful because of the intimate adhesion of the mass to the tympanic membrane. There was also extensive middle ear disease (cholesteatoma), which may have contributed to initial treatment failure. This highlights the importance of careful case selection for this procedure. Currently, the contraindications for VALE are unknown; therefore, we propose a larger prospective study to determine the indications and contraindications of this technique for aural mass excision. One may argue that if there is extensive middle ear disease, including bulla wall disease, TECALBO may be preferable in the first instance. The authors are aware of three other reports describing similar outcomes of VALE of aural masses in dogs. In one report, a 7-year-old Shih-tzu underwent excision of complex ceruminous adenomas using a diode laser (DLV-20, Asuka Medical Inc.) with multiple subsequent video-otoscopic therapies consisting of cleansing the ear canal with polyoxyethylene octylphenyl ether 0.5% (Nolvasan Otic, Kirikan, Ltd., Tokyo, Japan). The patient was cured of otitis media with no reoccurrence at 2 years’ follow-up (Usui et al., 2015). In another report, a 12-year-old Cavalier King Charles Spaniel underwent traction-avulsion of an aural polyp and vaporization of the stalk using a diode laser (DLV-20, Asuka Medical Inc.). This patient had no reoccurrence at follow-up 3 years and 8 months post procedure (Hoshino et al., 2022). A third study was conducted to evaluate the outcomes and reoccurrence of ceruminous gland tumors excised with biopsy and ablation with a CO2 laser. This study reported low reoccurrence for both ceruminous gland adenomas and adenocarcinomas in dogs and cats with minimal postoperative complications (Pieper et al., 2023). Although these reports are promising, larger studies are needed to determine the safety and efficacy of diode lasers, CO2 or Ho:YAG lasers for the excision of aural masses in dogs. When selecting the type of laser it is important that the surgeon is familiar with the interaction between the laser and tissue being excised. The target chromophore is the substance that absorbs the laser light and for most lasers, the target chromophore is water, hemoglobin, or melanin (Knappe et al., 2004). Diode and Ho:YAG lasers both have water as their target chromophore and can, therefore, be used on most tissues (Azadgoli and Baker, 2016). Based on the desired effect the laser beam can be focused to ablate or vaporize tissue or defocus to create coagulation (Azadgoli and Baker, 2016). One study that compared lasers for the treatment of hyperplastic nasal turbinates in humans reported superior tissue ablation and reduced deep tissue coagulation with the Ho:YAG laser compared with the diode laser (Sroka et al., 2007). A similar finding was reported by Seitz et al. (2007) when comparing the effect of different lasers on porcine kidney tissue both macroscopically and microscopically. Larger studies are needed to quantify whether one laser type is superior for the ablation of aural masses in dogs and what effect this has on complications and reoccurrence rates. The main limitation of this case series is the variation in the type of aural mass in each case, which limits extrapolation to other clinical cases. Future studies evaluating this reported technique in more cases of a specific type of mass are needed. Additionally, the excision technique varied between cases with some masses being removed by the polypectomy snare first and others being directly excised with the Ho:YAG laser. This highlights the importance of careful case selection and the potential risks of iatrogenic damage following direct excision of the mass using a laser. The authors concluded that VALE with a Ho:YAG laser is an effective, minimally invasive option for the removal of aural masses in dogs. Studies with larger populations, uniformity in mass type, and longer follow-up periods are needed to determine potential contraindications and to better quantify the outcomes and complications of this procedure. AcknowledgmentsNone reported. Conflict of interestThe authors declare that they have no conflicts of interest. No AI-assisted technologies were used in the generation of this manuscript. FundingThe authors have no funding to disclose. Authors contributionsA.P. reviewed the cases, prepared the figures, and wrote the manuscript. J.P.S. conceptualized the study and reviewed the manuscript. S.A.T. provided the figure images and reviewed the manuscript. Data availabilityThe data supporting the findings of this study are available from the corresponding author upon request. ReferencesAzadgoli, B. and Baker, R.Y. 2016. Laser applications in surgery. Ann. Transl. Med. 4, 452. Beckman, S.L., Henry, W.B. and Cecher, P. 1990. Total ear canal ablation combining bulla osteotomy and curettage in dogs with chronic otitis externa and media. J. Am. Vet. Med. Assoc. 196, 84–90. Coleman, K.A. and Smeak, D.D. 2016. Complication rates after bilateral versus unilateral total ear canal ablation with lateral bulla osteotomy for end-stage inflammatory ear disease in dogs: 79 ears. Vet. Surg. 45, 659–663. Greci, V. and Mortellaro, C.M. 2016. Management of otic, nasopharyngeal, and nasal polyps in cats and dogs. Vet. Clin. North Am. Small Anim. Pract. 46, 643–661. Greci, V., Vernia, E. and Mortellaro, C.M. 2014. Per-endoscopic trans-tympanic traction for the management of feline aural inflammatory polyps: a case review of 37 cats. J. Feline Med. Surg. 16, 645–650. Hoshino, T., Fukuda, S. and Nagata, M. 2022. Diode laser-assisted transcanal endoscopic removal of an aural polyp in the external auditory canal of a dog. Vet. Med. Sci. 8, 1862–1866. Knappe, V., Frank, F. and Rohde, E. 2004. Principles of lasers and biophotonic effects. Photomed. Laser Surg. 22, 411–417. Mason, L.K., Harvey, C.E. and Orsher, R.J. 1988. Total ear canal ablation combined with lateral bulla osteotomy for end-stage otitis in dogs: results in thirty dogs. Vet. Surg. 17, 263–268. Pieper, J.B., Noxon, J.O. and Berger, D.J. 2023. Retrospective evaluation of ceruminous gland tumors confined to the external ear canal of dogs and cats treated with biopsy and CO2 laser excision. J. Vet. Intern. Med. 37, 2385–2390. Schuldenfrei, M.D., Lam, A.T.H., Outerbridge, C.A., White, S.D. and Affolter, V.K. 2023. Evaluation of aural masses submitted as inflammatory polyps in 20 dogs (2000-2020). Vet. Dermatol. 34, 77–86. Seitz, M., Ackermann, A., Gratzke, C., Schlenker, B., Ruszat, R., Bachmann, A., Stief, C., Reich, O. and Sroka, R. 2007. Diode laser: ex vivo studies on vaporization and coagulation characteristics. Urologe A 46, 1242–1247. Smeak, D.D. 2011. Management of complications associated with total ear canal ablation and bulla osteotomy in dogs and cats. Vet. Clin. North Am. Small Anim. Pract. 41, 981–994. Spivack, R.E., Elkins, A.D., Moore, G.E. and Lantz, G.C. 2013. Postoperative complications following TECA-LBO in the dog and cat. J. Am. Anim. Hosp. Assoc. 49, 160–168. Sroka, R., Janda, P., Killian, T., Vaz, F., Betz, C.S. and Leunig, A. 2007. Comparison of long-term results after Ho:YAG and diode laser treatment of hyperplastic inferior nasal turbinates. Lasers Surg. Med. 39, 324–331. Usui, R., Okada, Y., Fukui, E. and Hasegawa, A. 2015. A canine case of otitis media examined and cured using a video otoscope. J. Vet. Med. Sci. 77, 237–239. | ||
| How to Cite this Article |
| Pubmed Style Prabakaran A, Sumner JP, Tyler SA. Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. Open Vet. J.. 2025; 15(6): 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 Web Style Prabakaran A, Sumner JP, Tyler SA. Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. https://www.openveterinaryjournal.com/?mno=248004 [Access: January 25, 2026]. doi:10.5455/OVJ.2025.v15.i6.61 AMA (American Medical Association) Style Prabakaran A, Sumner JP, Tyler SA. Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. Open Vet. J.. 2025; 15(6): 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 Vancouver/ICMJE Style Prabakaran A, Sumner JP, Tyler SA. Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. Open Vet. J.. (2025), [cited January 25, 2026]; 15(6): 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 Harvard Style Prabakaran, A., Sumner, . J. P. & Tyler, . S. A. (2025) Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. Open Vet. J., 15 (6), 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 Turabian Style Prabakaran, Adheip, Julia P. Sumner, and Sophie A. Tyler. 2025. Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. Open Veterinary Journal, 15 (6), 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 Chicago Style Prabakaran, Adheip, Julia P. Sumner, and Sophie A. Tyler. "Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs." Open Veterinary Journal 15 (2025), 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 MLA (The Modern Language Association) Style Prabakaran, Adheip, Julia P. Sumner, and Sophie A. Tyler. "Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs." Open Veterinary Journal 15.6 (2025), 2909-2914. Print. doi:10.5455/OVJ.2025.v15.i6.61 APA (American Psychological Association) Style Prabakaran, A., Sumner, . J. P. & Tyler, . S. A. (2025) Video otoscopy-assisted Holmium: yttrium-aluminum garnet laser excision of aural masses in four dogs. Open Veterinary Journal, 15 (6), 2909-2914. doi:10.5455/OVJ.2025.v15.i6.61 |

