




| Case Report | ||
Open Vet. J.. 2025; 15(7): 3369-3377 Open Veterinary Journal, (2025), Vol. 15(7): 3369-3377 Case Report Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament ruptureEunryel Nam1,2*, Madoka Amano1, Manabu Mochizuki1,3 and Muneki Honnami11Veterinary Medical Center, Graduate School of Agricultural and Life Sciences, The University of Tokyo, Tokyo, Japan 2Laboratory of Companion Animal Surgery, School of Veterinary Medicine, Rakuno Gakuen University, Ebetsu, Japan 3Laboratory of Veterinary Emergency Medicine, Graduate School of Agricultural and Life Sciences, The University of Tokyo, Tokyo, Japan *Corresponding Author: Eunryel Nam. Laboratory of Companion Animal Surgery, School of Veterinary Medicine, Rakuno Gakuen University, Ebetsu, Japan. Email: eunryelnam [at] gmail.com Submitted: 08/04/2025 Revised: 03/06/2025 Accepted: 23/06/2025 Published: 31/07/2025 © 2025 Open Veterinary Journal
ABSTRACTBackground: Cranial cruciate ligament rupture (CCLR) is a leading cause of lameness in dogs, often requiring surgical stabilization. Tibial plateau leveling osteotomy (TPLO) is a widely used procedure; however, postoperative instability, including the pivot shift phenomenon, can occur. This case highlights the need for additional stabilization techniques when TPLO alone is insufficient. Case Description: A 5-kg toy poodle presented with right hind limb CCLR. The tibial plateau angle (TPA) was 25°, and no injury was observed in the medial meniscus. TPLO was performed; however, postoperative instability due to the pivot shift phenomenon was observed. To restore joint stability, a lateral fabellotibial suture (LFTS) was placed. Eight weeks later, lameness developed in the left hind limb, and orthopedic examination confirmed CCLR with a TPA of 25° and an intact medial meniscus. LFTS was applied to the left stifle joint due to recurrent instability following TPLO. Postoperatively, stifle joint stability was regained in both hind limbs. Conclusion: While TPLO is an effective treatment for CCLR, some cases may require additional stabilization. This case suggests that LFTS can be a valuable adjunct for managing postoperative instability in small-breed dogs, improving surgical outcomes when the pivot shift phenomenon occurs. Keywords: Cruciate ligament rupture, Lateral fabellotibial suture, Pivot shift phenomenon, Tibial plateau leveling osteotomy, Toy-breed dog. IntroductionCranial cruciate ligament rupture (CCLR) is a frequently observed orthopedic condition in dogs. While CCLR is more prevalent in large-breed dogs, its incidence has been increasing among toy-breed dogs (Brioschi and Arthurs, 2021). Damage to the cranial cruciate ligament can lead to chronic complications such as meniscus detachment, tearing, and arthritis owing to cranial tibial subluxation and instability of the stifle joint. Osteotomy procedures, such as cranial tibial wedge osteotomy, tibial plateau leveling osteotomy (TPLO), and tibial tuberosity advancement, can restore the stability of the stifle joint (Comerford et al., 2013). Lameness caused by CCLR in toy-breed dogs can be managed conservatively through the administration, such as the administration of non-steroidal anti-inflammatory drugs, weight loss, and cage rest, as their body weight (<15 kg) is lower than that of medium and large breeds (Kwananocha et al., 2024). Notably, TPLO has been shown to shorten the period of postoperative lameness even in toy-breed dogs (Knight and Danielski, 2018; Tikekar et al., 2022; Schuenemann and Kaczmarek, 2023). A combination of TPLO and lateral fabellotibial suture (LFTS) has been widely used to limit the postoperative instability of the stifle joint in large-breed dogs with CCLR (Schaible et al., 2017). These integrated surgical procedures temporarily promote adequate periarticular fibrosis, decrease cranial tibial subluxation, and strengthen the hamstring muscles, thereby maintaining long-term stability and facilitating functional recovery of the stifle joint postoperatively (Harasen, 2008). This report presents a case wherein a greater postoperative stability of the stifle joint was achieved by using a combination of TPLO and LFTS in a toy-breed dog. Tibial subluxation and rotation were observed post-TPLO; however, the placement of an additional LFTS on the stifle joint restored the stability of the joint successfully. Case DetailsA 12-year-old castrated male toy poodle weighing 5 kg jumped off the couch 1 month prior and was unable to support weight on his right hind limb. The dog was taken to a local veterinary hospital after 2 days, where radiography revealed CCLR. Despite 3 weeks of cage rest and the analgesic administration, lameness persisted in the right hind limb. Consequently, the owners sought treatment at the Veterinary Medical Center at the University of Tokyo to restore full limb function. Weak weight-bearing lameness was observed in the right hind limb, accompanied by pain on hyperextension and swelling of the stifle joint. A 1-cm decrease in the right thigh diameter relative to the left was observed following muscle girth assessment with a flexible measuring tape. Orthopedic examination revealed cranial displacement of the tibia without medial or lateral patellar luxation. The results of the cranial drawer and tibial compression tests were positive. Radiography of the right stifle joint indicated infrapatellar fat pad signs and cranial tibial luxation (Fig. 1A). No obvious angular limb deformities were observed (Fig. 1A and D). Ultrasonography of the stifle joints (ARIETTA Prologue; Fujifilm Co., Japan; 18 MHz linear probe) revealed a complete CCLR, severe joint effusion, and medial buttress in the right stifle joint with no injury to the medial meniscus (Fig. 2A–C). Furthermore, partial CCLR and mild joint effusion were observed in the left stifle joint. The owner was advised that surgical intervention was necessary to restore the stability of the stifle joint of the right hind limb and that the partial rupture of the ligament in the left hind limb posed a significant risk of progressing to a complete tear in the future. TPLO was performed for the treatment of the right CCLR after obtaining consent from the owner. Before surgery, the tibial plateau angle (TPA), the distance from the insertion of the patellar ligament to the osteotomy perpendicular to the cranial border of the tibia (D1), and the distance between the insertion of the patellar ligament and exit of the cranioproximal osteotomy (D2) were measured as described in a previous report (Fujino et al., 2020). TPA was measured as 25° on the preoperative radiographs, and a 2.4-mm TPLO plate (VP4404-R3; DePuy Synthes Japan, Japan) was selected for TPLO. D1 and D2 were measured as 7.5 and 8.2 mm, respectively. Before surgery, atropine (Atropine Sulfate Injection 0.5mg; NIPRO Co., Ltd., Japan) was administered intravenously. Anesthesia induction was achieved using intravenous propofol (Mairan 1% propofol injection; MSD Animal Health K.K., Japan) and maintained with 1%–2% isoflurane (Isofuru®; Zoetis Japan K.K., Japan) in oxygen. A continuous infusion of fentanyl at 10 μg/kg/hr (Fentanyl Injection 0.5 mg; Janssen Pharmaceutical K.K., Japan) and ketamine at 1 mg/kg/hr (Ketalar®; Daiichi Sankyo Propharma Co., Ltd., Japan) was maintained. Cefazolin sodium injection (Nichi-Iko Pharmaceutical Co., Ltd., Japan) was administered intravenously at 20 mg/kg 30 minutes before surgery and every 1.5 hours thereafter during the perioperative period. The right pelvic limb was clipped and prepared aseptically. Peripheral blockade of the femoral and sciatic nerves was performed using bupivacaine injection (Marcaine®; Aspen Japan K.K., Japan) at 0.25% and 0.1 ml/kg under ultrasonographic guidance. An incision was made along the medial parapatellar region to examine the medial meniscal lesions and assess the integrity of the cranial cruciate ligament. Consistent with the ultrasonographic findings, the cranial cruciate ligament was found to be completely ruptured, and no medial meniscal injury was identified intraoperatively. No extraction was necessary as only minimal remnants of the ligament were present. The positions of D1 and D2 were marked using electrocautery after measurement. A 15-mm TPLO saw manufactured by Johnson & Johnson K.K. (DePuy Synthes, Japan) was used for osteotomy. A Kirschner wire (1.5 mm diameter) was inserted into the proximal bone segment subsequently and rotated until achieving a postoperative TPA of 5°. Another Kirschner wire (1.0 mm in diameter) was inserted through the proximal part of the tibial tuberosity to the segment for temporary fixation. The Kirschner wires were removed after securing the plate, cortical screws, and locking screws at the predetermined bone site and confirming the stabilization of the segment. During the tibial compression test post-TPLO plate placement, tibial cranial subluxation and internal rotation occurred intraoperatively. An LFTS was placed using a No. 3 monofilament nylon and an LFTS needle (BEAR Medic Co., Japan) as follows: a single strand of LFTS was passed around the lateral femoral fabella, cut at the needle, and both ends passed under the patellar ligament. One end of the strand was then passed proximally to the cranial screw under the TPLO plate, and the other end was passed distally through the same screw (Fig. 3A). The surgeon’s knot was ligated to the caudal side of the TPLO plate (Fig. 3B). The resolution of the tibial dislocation was confirmed with a second tibial compression test. The incision was closed in three layers, and two orthogonal postoperative radiographs were acquired to evaluate the position of the implants and bone fragments. A modified Robert Jones bandage (soft padded bandage) was applied under general anesthesia after postoperative radiography (Fig. 1B and E) and maintained for 2 days. The non-steroidal anti-inflammatory agent firocoxib (Previcox®; Boehringer Ingelheim Animal Health Japan Co., Ltd., Japan) was administered orally at 5 mg/kg every 24 hours, and cefazolin (Cefaclear®; Kyoritsu Seiyaku Co., Japan K.K., Japan) at 20 mg/kg every 12 hours for 5 days postoperatively. Lameness evaluation, client satisfaction, and radiographic follow-up were performed at 10 days and 4, 8, and 14 weeks postoperatively.
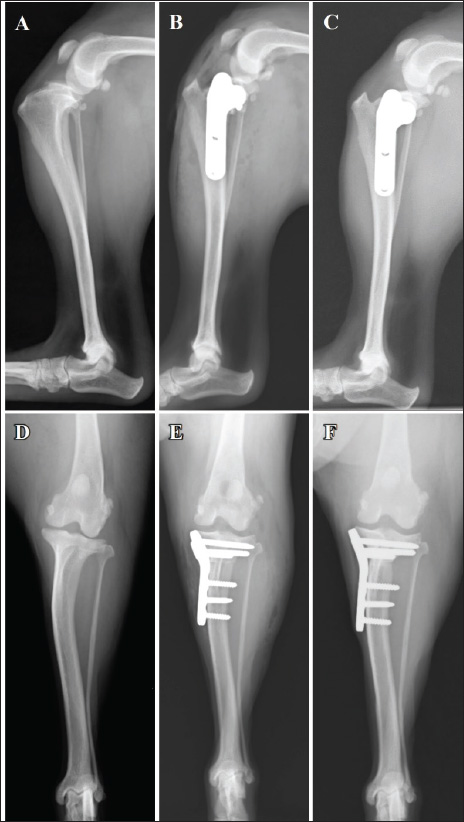
Fig. 1. Mediolateral radiographs (A–C) and caudocranial radiographs (D–F) of the right limb. The infrapatellar fat pad sign and cranial tibial luxation at the first visit (A). Absence of angular limb deformities (D). Placement of a 2.4-mm TPLO plate (B and E). No osteotomy line at the 14-week follow-up (C). No evidence of dislocation at the 14-week post-TPLO (F) follow-up.
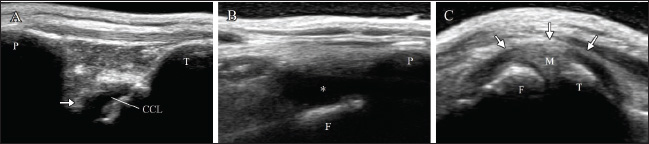
Fig. 2. Ultrasonography of the right stifle joint at the first visit. Complete rupture of the cranial cruciate ligament (arrow, A) and severe joint effusion (asterisk, B) can be observed. Although the medial buttress (arrow, C) can be visualized, the caudal horn of medial meniscus shows no damages (C). CCL=cranial cruciate ligament; F=femur; M=medial meniscus; P=patella; T=tibia.
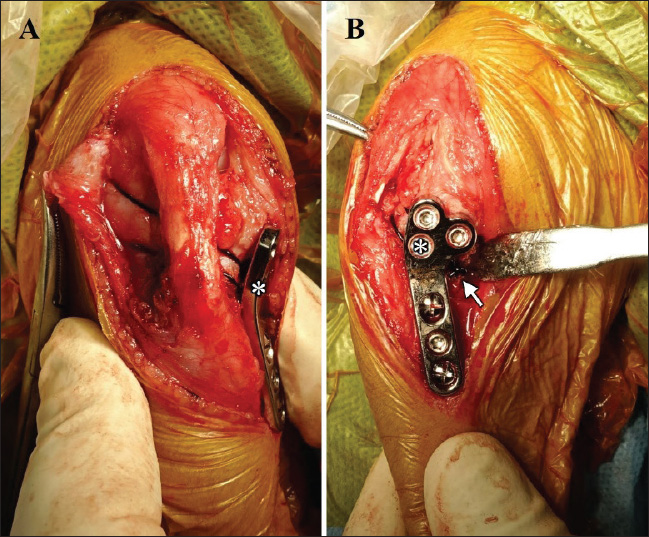
Fig. 3. LFTS following the TPLO plate placement in the right hind limbs. The nylon suture is passed around the lateral femoral fabella. Both ends of the suture are passed under the patella ligament subsequently. One end of the suture is passed proximally, and the other end of the suture is passed distally to the cranial screw (asterisk) under the TPLO plate (A and B). The surgeon’s knot is ligated on the caudal side of the TPLO plate (arrow, B). Left weight-bearing lameness with pain upon hyperextension and swelling in the left stifle joint were reported 8 weeks post-surgery of the right limb. The results of the cranial drawer and tibial compression tests performed as a part of the orthopedic examination of the left limb were positive. Radiography revealed the presence of the infrapatellar fat pad sign and cranial tibial luxation at the left stifle joint, with no obvious angular limb deformities (Fig. 4A and D). Ultrasonography of the left stifle joint revealed complete CCLR, moderate joint effusion, and medial buttress without damage to the caudal horn of the medial meniscus (Fig. 5A–C). Preoperative radiographs revealed a TPA of 25°. A 2.4-mm TPLO plate (VP4404-L3; DePuy Synthes Japan, Japan) was selected for TPLO. Identical to the measurements for the right limb, D1 and D2 for the left limb were 7.5 and 8.2 mm, respectively. Arthroscopy and surgery were performed under general anesthesia. Arthroscopy revealed complete CCLR and medium-stage angiogenesis of the caudal cruciate ligament with no damage to the medial meniscus observed (Fig. 6A). A No. 11 blade was used to remove the remaining portion of the cranial cruciate ligament. TPLO of the left limb was performed as described previously. LFTS was placed in the same manner as described previously owing to tibial cranial subluxation and internal rotation intraoperatively post-TPLO (Fig. 6B and C). Subluxation or rotation was not observed following the second tibial compression test. The medications administered post-surgery of the right limb were also prescribed based on postoperative radiographs (Fig. 4B and E). Postoperative radiography revealed that the TPA was 5° on both sides. The owner was satisfied with the postoperative weight-bearing ability of the limb while walking at the 4-week follow-up visit. A faint osteotomy line was visible, and radiography revealed aligned and positioned TPLO plates and bone segments with no displacement. No tibial translocation was detected during the compression test. The dog was able to use its right hind limb without any discomfort at the 8-week follow-up visit. The osteotomy line had disappeared, and radiography revealed aligned TPLO implants. Tibial translocation was not detected during the compression test. Minimal discomfort upon waking up was reported at the 14-week follow-up visit for the right limb (4-week follow-up for the left limb); lameness was not observed while walking or trotting. The tibial compression test results were negative for both limbs, and the rotated bone fragment showed complete fusion with the tibia of the right limb (Fig. 1C and F). A faint osteotomy line was observed in the tibia of the left limb. Radiography revealed no dislocation of the bone or the TPLO implants on the right or left sides. The owner was pleased with the significant improvement in walking ability. By the 13-week follow-up visit osteotomy line in the left limb was not visible, with no residual discomfort or lameness in either limb. The osteotomy line was not apparent owing to bone union (Fig. 4C). The implant alignment and bones remained stable (Fig. 4F). DiscussionBoth limbs exhibited tibial instability post-TPLO in this patient. Although no injury of medial meniscus in the right limb was identified on gross inspection, arthroscopy in the left limb was performed to clarify the cause of the pivot shift phenomenon post-TPLO in the right limb. The pivot shift phenomenon was observed in the left limb following TPLO despite arthroscopy revealing no damage to the meniscus. Further, the TPA of both limbs was identical before and after TPLO. The pivot-shift phenomenon, characterized by uncontrolled internal rotation of the tibia while bearing weight post-TPLO, was noted (Knight and Danielski, 2018). The specific cause of this phenomenon remains unknown; however, it may be attributed to medial meniscectomy, angular deformity, tibial torsion, or excessive internal rotation of the tibia, either independently or in combination (Pozzi et al., 2006; Thieman et al., 2006; Boudrieau, 2009; Knight and Danielski, 2018). Although meniscectomy has been reported to influence the pivot shift phenomenon regardless of changes in TPA post-TPLO, it was not performed in this case (Kim et al., 2012). Restoration of stifle joint stability which retains lameness after TPLO-related pivot shift typically occurs within approximately 4–6 months or may necessitate additional surgery (Wheeler et al., 2003; Gatineau et al., 2011; Bureau, 2017; Knight et al., 2017). Although these findings are specific to large-breed dogs, the pivot shift phenomenon can also occur in toy-breed dogs without meniscal damage in this study. LFTS was applied to both limbs to mitigate internal tibial rotation, as the pivot-shift phenomenon was observed following TPLO plate placement. In addition, lameness or tibial subluxation was not observed for 5 months postoperatively in the right limb. This finding indicates that a combination of TPLO and LFTS may improve stifle joint stability in toy-breed dogs exhibiting intraoperative pivot shift without identifiable cause. The optimal combination of LFTS attachment sites and stifle angles for suture placement varies among dogs (Witte, 2015). To preserve the tension of the LFTS suture and maintain the stifle joint stability, the surgeon’s knot was placed between the caudal side of the TPLO plate and the tibial bones after looping the strand around the cranial screw. Alternatively, passing the strand above and below the plate and ligating the knot on the surface of the plate may also help prevent the pivot shift phenomenon. Nevertheless, we placed the knot on the side of the plate to minimize irritation to the skin covering the plate, as toy-breed dogs generally have thinner skin over the tibial bone compared to large breed dogs. Meanwhile, placing the surgeon’s knot under the plate increases the gap between the tibial bone and the plate, and may exacerbate the instability of the fixation.
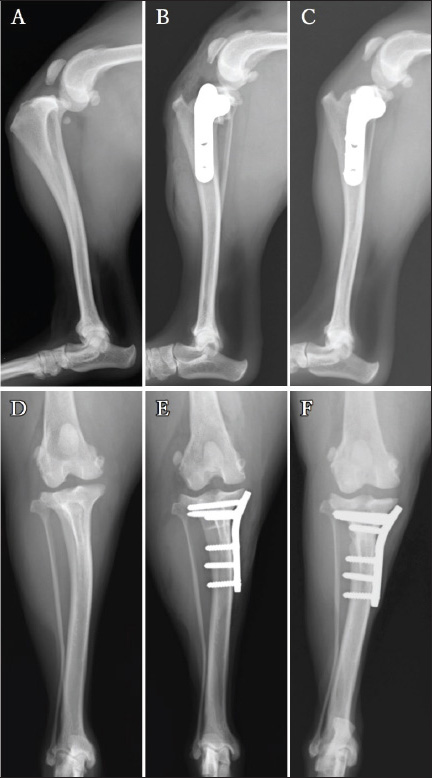
Fig. 4. Mediolateral radiographs (A–C) and caudocranial radiographs (D–F) of the left limb. The infrapatellar fat pad sign and cranial tibial luxation at the left stifle joint before the surgery (A). No obvious angular limb deformity can be visualized (D). A postoperative radiograph acquired after the 2.4-mm TPLO plate placement (B and E). The tibial bone and bone fragment are completely fused at 13 weeks post-surgery (C). Additionally, the caudocranial radiograph at the 13-week (F). Follow-up visit shows no sign of dislocation of the implants.
Fig. 5. Ultrasonography of the left stifle joint at 8 weeks after surgery on the right limb. The joint shows complete rupture of cranial cruciate ligament (arrow, A), moderate joint effusion (asterisk, B), and the medial buttress (arrow, C). The caudal horn of medial meniscus shows no injury (C). CCL=cranial cruciate ligament; F=femur; M=medial meniscus; P=patella, T=tibia.
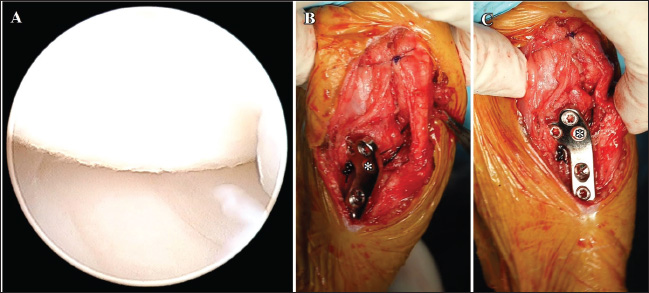
Fig. 6. Arthroscopic image of the medial meniscus and LFTS following the TPLO plate placement on the left limb. The medial meniscus is intact (A). The nylon suture is passed around the lateral femoral fabella. Both ends of the suture are passed under the patella ligament. One end of the suture is passed proximally, and the other end of the suture is passed distally to the cranial screw (asterisk) under the TPLO plate (B and C). The surgeon’s knot is ligated on the caudal side of the TPLO plate (arrow, C). F=femur; M=medial meniscus; T=tibia. A bone tunnel is typically created in the tibial tuberosity to facilitate the passage of the LFTS strand (Knight and Danielski, 2018). The spatial flexibility of the tibia following installation of the TPLO plate in toy-breed dogs is less than that observed in middle and large-breed dogs. The bone tunnel could increase the incidence of side effects such as tibial tuberosity fractures. To minimize iatrogenic risks, we employed the modified LFTS technique described earlier. This fixation strategy may provide a feasible substitute in small dogs where traditional tunnel-based techniques pose a higher complication risk. We applied No. 3 monofilament nylon suture owing to its documented tensile strength and established suitability for extracapsular stabilization in small-breed dogs. The application of LFTS alone may require a stronger strand or a greater number of strands. However, the TPLO plate had already controlled the cranial tibial thrust. Therefore, we selected the No. 3 suture, which provides tensile strength nearly double the dog’s body weight. The combination of TPLO and LFTS procedures is associated with an increased risk of complications, such as infection or tibial tuberosity fractures (Schaible et al., 2017). Furthermore, suture materials, such as nylon, placed around the joint during LFTS, could increase the possibility of infection compared with a single TPLO. Persistent postoperative lameness caused by implant infection potentially requires a second surgery to remove the implant. In this case, antibiotics were administered for 5 days post-surgery to prevent infection. Although the placement TPLO plate and the single strand of the LFTS could enhance stifle joint stability with CCLR, further studies must be conducted to determine the specific cause of the pivot shift phenomenon post-TPLO in toy breeds. In addition, the single stand of the LFTS demonstrated sufficient strength to maintain the stability of the stifle joint for up to 5 months after the TPLO surgery in dog weighing under 6 kg. However, stronger LFTS materials such as thicker sutures or double strands may need to guarantee adequate stabilization in toy-breed dogs weighing over 6-kg toy-breed dogs. As this report describes only a single case, additional case studies in toy-breed dogs are necessary to establish appropriate LFTS materials and fixation methods. ConclusionThe findings of this report indicate that the combination of TPLO and LFTS effectively restores the stability of the stifle joint in large and toy-breed dogs. To the best of our knowledge, this is the first report to demonstrate the effectiveness of the combination of TPLO and LFTS in toy-breed dogs (<6 kg) with CCLR. AcknowledgmentsWe would like to thank Editage (www.editage.com) for its English language editing services. Conflict of interestThe authors declare no conflicts of interest. FundingThis work was supported by Rakuno Gakuen University. Author’s contributionsNam ER and Honnami contributed equally to this study. Conceptualization: Nam ER, Honnami M; Data curation: Nam ER, Honnami M; Funding acquisition: Nam ER; Methodology: Honnami M, Amano M; Supervision: Mochizuki M; Writing—original draft: Nam ER; Writing—review and editing: Nam ER, Honnami M. Data availabilityAll data supporting the findings of this study are available within the manuscript. ReferencesBoudrieau, R.J. 2009. Tibial plateau leveling osteotomy or tibial tuberosity advancement? Vet. Surg. 38, 1–22. Brioschi, V. and Arthurs, G.I. 2021. Cranial cruciate ligament rupture in small dogs (<15 kg): a narrative literature review. J. Small Anim. Pract. 62, 1037–1050. Bureau, S. 2017. Owner assessment of the outcome of tibial plateau levelling osteotomy without meniscal evaluation for treatment of naturally occurring cranial cruciate ligament rupture: 130 cases (2009 to 2013). J. Small Anim. Pract. 58, 468–475. Comerford, E., Forster, K., Gorton, K. and Maddox, T. 2013. Management of cranial cruciate ligament rupture in small dogs: a questionnaire study. Vet. Comp. Orthop. Traumatol. 26, 493–497. Fujino, H., Honnami, M. and Mochizuki, M. 2020. Preoperative planning for tibial plateau leveling osteotomy based on proximal tibial width. J. Vet. Med. Sci. 82, 661–667. Gatineau, M., Dupuis, J., Planté, J. and Moreau, M. 2011. Retrospective study of 476 tibial plateau levelling osteotomy procedures. Rate of subsequent ‘pivot shift’, meniscal tear and other complications. Vet. Comp. Orthop. Traumatol. 24, 333–341. Harasen, G. 2008. Canine cranial cruciate ligament rupture in profile: 2002–2007. Can. Vet. J. 49, 193–194. Kim, S.E., Lewis, D.D. and Pozzi, A. 2012. Effect of tibial plateau leveling osteotomy on femorotibial subluxation: in vivo analysis during standing. Vet. Surg. 41, 465–470. Knight, R. and Danielski, A. 2018. Long-term complications following tibial plateau leveling osteotomy in small dogs with tibial plateau angles > 30°. Vet. Rec. 182, 461. Knight, R.C., Thomson, D.G. and Danielski, A. 2017. Surgical management of pivot-shift phenomenon in a dog. J. Am. Vet. Med. Assoc. 250, 676–680. Kwananocha, I., Akaraphutiporn, E., Upariputti, R., Lekchareonsuk, C. and Wangdee, C. 2024. Short-term outcomes of cranial cruciate ligament rupture treated surgically with tibial plateau leveling osteotomy or nonsurgically in small-breed dogs weighing less than 10 kg. J. Vet. Med. Sci. 86, 428–435. Pozzi, A., Kowaleski, M.P., Apelt, D., Meadows, C., Andrews, C.M. and Johnson, K.A. 2006. Effect of medial meniscal release on tibial translation after tibial plateau leveling osteotomy. Vet. Surg. 35, 486–494. Schaible, M., Ben-Amotz, R., Caceres, A., Payton, M., Segev, Y. and Shani, J. 2017. Combined tibial plateau leveling osteotomy and lateral patellotibial suture for cranial cruciate ligament rupture with severe rotational instability in dogs. J. Small Anim. Pract. 58, 219–226. Schuenemann, R. and Kaczmarek, J. 2023. Tibial Plateau Leveling Osteotomy in small and large breed dogs: a comparative retrospective study of complications and outcomes. Tierarztl. Prax. Ausg. K. Kleintiere Heimtiere. 51, 6–14. Thieman, K.M., Tomlinson, J.L., Fox, D.B., Cook, C. and Cook, J.L. 2006. Effect of meniscal release on the rate of subsequent meniscal tears and owner-assessed outcome in dogs with cruciate disease treated with tibial plateau leveling osteotomy. Vet. Surg. 35, 705–710. Tikekar, A., De Vicente, F., McCormack, A., Thomson, D., Farrell, M., Carmichael, S. and Chase, D. 2022. Retrospective comparison of outcomes following tibial plateau levelling osteotomy and lateral fabello-tibial suture stabilisation of cranial cruciate ligament disease in small dogs with high tibial plateau angles. N. Z. Vet. J. 70, 218–227. Wheeler, J.L., Cross, A.R. and Gingrich, W. 2003. In vitro effects of osteotomy angle and osteotomy reduction on tibial angulation and rotation during the tibial plateau-leveling osteotomy procedure. Vet. Surg. 32, 371–377. Witte, P.G. 2015. Tibial anatomy in normal small breed dogs including anisometry of various extracapsular stabilizing suture attachment sites. Vet. Comp. Orthop. Traumatol. 28, 331–338. | ||

| How to Cite this Article |
| Pubmed Style Nam E, Amano M, Mochizuki M, Honnami M. Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. Open Vet. J.. 2025; 15(7): 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 Web Style Nam E, Amano M, Mochizuki M, Honnami M. Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. https://www.openveterinaryjournal.com/?mno=252798 [Access: June 27, 2026]. doi:10.5455/OVJ.2025.v15.i7.50 AMA (American Medical Association) Style Nam E, Amano M, Mochizuki M, Honnami M. Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. Open Vet. J.. 2025; 15(7): 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 Vancouver/ICMJE Style Nam E, Amano M, Mochizuki M, Honnami M. Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. Open Vet. J.. (2025), [cited June 27, 2026]; 15(7): 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 Harvard Style Nam, E., Amano, . M., Mochizuki, . M. & Honnami, . M. (2025) Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. Open Vet. J., 15 (7), 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 Turabian Style Nam, Eunryel, Madoka Amano, Manabu Mochizuki, and Muneki Honnami. 2025. Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. Open Veterinary Journal, 15 (7), 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 Chicago Style Nam, Eunryel, Madoka Amano, Manabu Mochizuki, and Muneki Honnami. "Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture." Open Veterinary Journal 15 (2025), 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 MLA (The Modern Language Association) Style Nam, Eunryel, Madoka Amano, Manabu Mochizuki, and Muneki Honnami. "Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture." Open Veterinary Journal 15.7 (2025), 3369-3377. Print. doi:10.5455/OVJ.2025.v15.i7.50 APA (American Psychological Association) Style Nam, E., Amano, . M., Mochizuki, . M. & Honnami, . M. (2025) Correction of pivot shift phenomenon following tibial plateau leveling osteotomy using lateral fabellotibial suture in a toy-breed dog with cranial cruciate ligament rupture. Open Veterinary Journal, 15 (7), 3369-3377. doi:10.5455/OVJ.2025.v15.i7.50 |

