




| Research Article | ||
Open Vet. J.. 2026; 16(1): 363-371 Open Veterinary Journal, (2026), Vol. 16(1): 363-371 Research Article Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signsShadi J. Ireifej1*, Samantha L. Morello2 and Marty Lesser3,41VetTriage, Las Vegas, NV, USA 2Center for Veterinary Business and Entrepreneurship, Cornell University College of 3Statistical Consulting, East Rockaway, NY, USA 4Departments of Molecular Medicine & Occupational Medicine, Epidemiology and *Corresponding Author: Shadi J. Ireifej. VetTriage, Las Vegas, NV, USA. Email: shadi.ireifej [at] vettriage.com Submitted: 23/07/2025 Revised: 22/11/2025 Accepted: 11/12/2025 Published: 31/01/2026 © 2025 Open Veterinary Journal
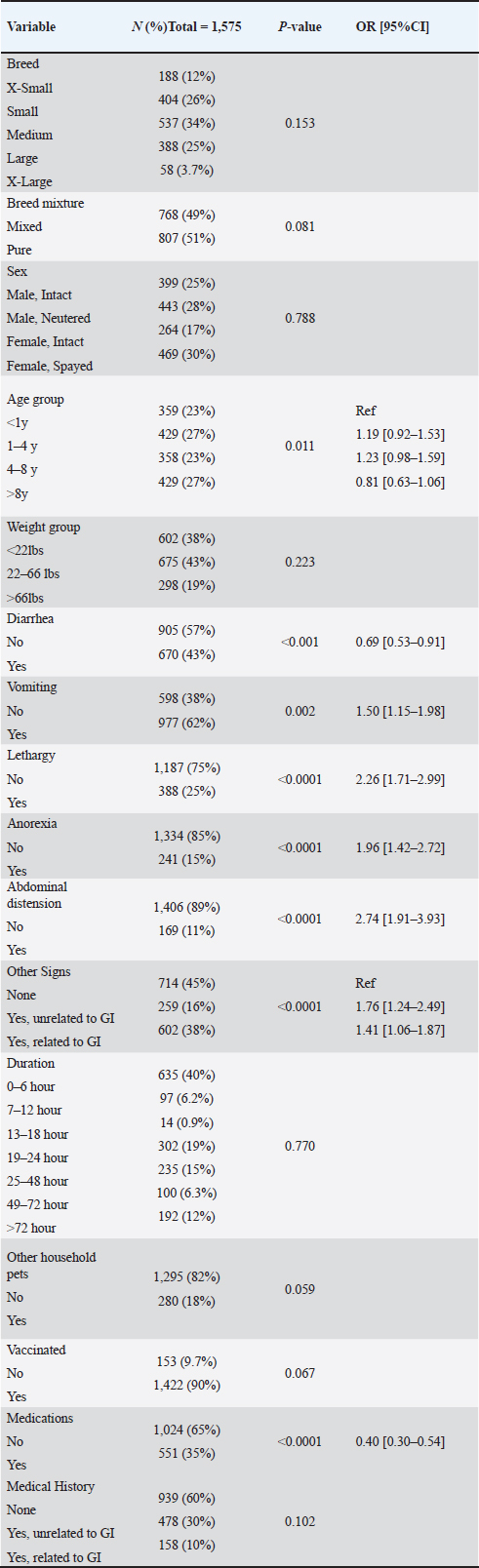
AbstractBackground: Veterinary telehealth can provide veterinary care to various species, geographic locations, client demographics, and practice types. Factors influencing the veterinarian decision when teletriage and teleadvice are administered to a large number of dogs with gastrointestinal (GI) signs have not been previously reported. Aim: To report on dogs evaluated via a veterinarian-led teletriage and teleadvice synchronous video service for GI signs to determine factors associated with referral recommendation for in-person emergency (ER) evaluation. Methods: The number of animals was 1,575 dogs. Case records summarizing video telehealth evaluations of dogs presenting for GI symptoms performed by veterinarians were reviewed, and data on signalment, history, and clinical signs were collected. Visit outcome was recorded as to whether the patient received a recommendation for an in-person ER referral. The primary statistical objective was to determine which variables were significantly associated with ER referral. Results: Overall, 23% of the cases presented were recommended for in-person ER referral. Vomiting was the most common clinical complaint (62%) and was associated with a 50% greater odds of referral recommendation. Diarrhea was present in 43% of patients and was associated with a 31% lower odds of referral. Abdominal distention and lethargy were associated with the greatest increase in odds of referral recommendation (174% and 126%, respectively). Multivariable logistic regression identified that vomiting, lethargy, anorexia, the presence of other clinical signs, and abdominal distention were significantly associated with ER referral, and a current medication history was negatively associated with ER referral. Conclusion: Dogs with vomiting alone, with a combination of abdominal distention, or with a combination of lethargy, anorexia, abdominal distention, and other clinical signs, confirmed by a veterinarian-led synchronous video teleadvice and teletriage service, have increased odds of being referred to an emergency facility compared with dogs without these clinical signs. Keywords: Teletriage, Teleadvice, Dogs, Gastrointestinal. IntroductionVeterinary telehealth can provide veterinary care to various species, geographic locations, client demographics, and practice types. Telehealth has existed for many years in the human field, yet it has only evolved in the veterinary field within the last decade (Cushing, 2022). As defined by the American Veterinary Medical Association (AVMA), telehealth “is the overarching term that encompasses all uses of technology to deliver health information, education, or care remotely [and] can be divided into categories based on who is involved in the communication (AVMA, 2024a,b).” One such category is teletriage, defined by the AVMA as “the safe, appropriate, and timely assessment and management (immediate referral to a veterinarian or not) of animal patients, under conditions of uncertainty and urgency, via electronic consultation with their owners. No diagnosis is rendered, and a veterinarian-client-patient relationship (VCPR) is not required (AVMA, 2024a,b).” The AVMA defines teleadvice as “the provision of any health information, opinion, guidance, or recommendation concerning prudent future actions that are not specific to a particular patient’s health, illness, or injury,” followed by proposed limitations of this category of telehealth (AVMA, 2024a,b). The current statutes characterizing the definition, utility, and breadth of veterinary telehealth, including its subcategories, vary by state and are undergoing constant change, both as demand grows and as veterinarians and lawmakers deliberate on the requirements for establishing a VCPR. The AVMA telehealth guidelines describe teletriage as providing a method for a veterinarian to assess an animal’s condition through telehealth and/or, more specifically, in an effort to determine the level of urgency of a patient’s condition as to whether immediate referral to a veterinarian is indicated (AVMA, 2024a,b). Such assessment typically uses visual (e.g., photographs and video) information in addition to a thorough history and accounting of clinical signs (e.g., verbal and written). The advice administered by a veterinarian via telehealth in such a context is known as “teleadvice”; it includes providing any health information, opinion, or guidance that is not specific to an animal patient’s health, illness, or injury, and it is not intended to diagnose, prognosticate, or treat the patient. Overall, the essence of teletriage and teleadvice is to administer advice regarding a patient’s status, including the need for referral under uncertainty and urgency. The availability of veterinary emergency (ER) care has grown substantially over the last two decades (Bain et al., 2019). In addition to the increasing use of technology to deliver medical advice, the COVID-19 pandemic and its associated effects led to one of the busiest times in veterinary ER care (Wayne and Rozanski, 2020; Finstad et al., 2023). Staffing challenges have emerged due to a combination of increases in unfilled veterinary ER positions and patientsseeking ER care, which can create a bottleneck to servicing the number of animals that seek care (Booth et al., 2021). While emergency care is most rigorously described as services “necessary to save life or relieve suffering”, many patients presenting to an ER may not require such critical intervention (AVMA, 2024a,b). This is analogous to a study in the human literature, where in 2022 the proportion of hospital admissions from nonurgent ER visits, severe ER visits, and critical ER visits resulting in admission was 0.5%, 8.1%, and 37.5%, respectively (Ruxin et al., 2023). When executed appropriately by experienced veterinarians who can visually evaluate the patient in real-time, teletriage and teleadvice could be highly effective in differentiating the patients most in need of immediate veterinary services and presumably have clear benefits over asynchronous or low-quality methods, such as text, chat, or email, because of the time-sensitive and urgent nature of triage. Our hypotheses are that there would be a minority of dogs for whom in-person emergency evaluation would be recommended, and of those dogs that were recommended immediate in-person evaluation on an emergency basis, there would be one or more specific gastrointestinal (GI) clinical signs in those dogs that would have been more likely to influence the televeterinarian’s decision on that recommendation. Studies evaluating the utility and outcome of veterinary telehealth, and specifically teletriage, are limited despite the increasing use of these types of services (Ireifej and Krol, 2023). This study aimed to test our hypotheses by reviewing a large population of dogs presenting for virtual evaluation of GI symptoms by veterinarians via a proprietary synchronous veterinary video telehealth platform for teletriage and teleadvice. GI symptoms were selected because this category of clinical signs is among the most commonly observed in emergency veterinary medicine (Parr and Otto, 2013; Saito and Rhoads, 2021). Our objectives were 1) to report the proportion of dogs whose teletriage examination resulted in the recommendation of referral for in-person emergency evaluation and treatment, and 2) to determine which clinical signs were associated with the greatest odds of being recommended for Materials and MethodsTelehealth examinationA database of cases presented for teletriage and teleadvice service to VetTriage, LLC (Las Vegas, Nevada) was used to collect data for this study. VetTriage uses a novel synchronous teletriage and teleadvice video teleconferencing platform to consult with clients on an emergency basis by a United States-licensed Doctor of Veterinary Medicine (DVM) and services all 50 states. All veterinarians are experienced practitioners (e.g., one decade or more of clinical experience) with expertise across a wide range of species and who are trained specifically in how to execute a teletriage evaluation. Animal owners (clients) are directed to the platform through their primary veterinary care center for emergency triage purposes, or they may choose to use the service on their own via the Internet. All clients must acknowledge the legal and ethical limitations of veterinary telehealth before engaging in teleconferencing with the DVM. A disclaimer presenting language pertaining to the VCPR and explaining the medical, ethical, and legal junctions of the VCPR as they currently stand (2019-present) is supplied to every client. VCPR is not established with clients as it is not required to administer teletriage or teleadvice (AVMA, 2024a,b). All animal and pet caretakers included in this study requested teleconferencing on their own accord for the purpose of teletriage and not for the purposes of the study. Veterinarian training consisted of a combination of many years of in-person clinical experience, as well as performing thousands of live video sessions on the platform. Additionally, internal protocols are designed to supplement the veterinarian’s educational benefit. Owing to the novel nature of this platform, no equivalent validated protocols exist in the veterinary literature. As such, these protocols were initially a “proof of concept” that became validated internally over time, examined across approximately 200,000 sessions over the platform’s existence. Finally, a library of real video sessions was recorded for the veterinarian’s education, depicting the methodologies that can be used to leverage the hands of the pet owner to physically manipulate the pet for the purposes of veterinary assessment (e.g., direct palpation of specific portions of the animal’s body). Selected training video sessions were based on the most common scenarios seen on this virtual platform, including, but not limited to, GI, ocular, and dermatologic cases as training examples. Considering the entire onboarding and training process of the televeterinarians on this platform, the approximate number of hours required to commit to and complete this training is 12 hours. The telehealth consultation between the televeterinarian and the client/pet owner contained no time limit and was left to the discretion of the televeterinarian, averaging 22 minutes per video session. Following the telehealth consultation, the consulting DVM creates a full summary of the telehealth evaluation, including signalment, history, clinical signs, video examination findings, and triage decision and advice given. The summary is shared directly with the client, the client’s primary veterinary care provider (if provided), and the emergency care provider or on-call DVM to whom the patient has been referred when necessary. Patients who are not recommended for emergency care are often advised to use any combination of supportive and over-the-counter therapeutics that do not require a prescription, and therefore, a VCPR, as appropriate based on the judgment of the consulting DVM, along with monitoring that the client can perform for the pet’s situation. All clients are encouraged to follow up with their primary veterinarian within 24 hours or at their next available appointment. Case selection and data collectionAll appropriate video session records were pulled for subsequent case review for the study’s purposes. Case records between 4/5/2020 and 11/17/2020 (2,043 records, total); 1/1/2021 and 12/2/2021 (7,976 records, total), and 1/1/2023 and 1/26/2023 (1,090 records, total) were manually reviewed for inclusion in this study. Three separate date windows were randomly selected for review by three different independent reviewers trained in the selection criteria, with an end goal of collecting a minimum of 1,500 cases for inclusion. A case was considered eligible for inclusion if the following criteria were met: (1) a complete telehealth record, (2) canine species, and (3) history and clinical signs attributed to the GI system, including one or more of the following: vomiting, diarrhea, abdominal distention, and anorexia. Data collected included breed (extra-small, small, medium, large, extra-large, based on American Kennel Club guidelines) (American Kennel Club, 2024), breed mixture (pure, mixed); age group (<1yr, 1-<4yrs, 4-<8yrs, >8 yrs), weight group (<22lbs, 22–66lbs, >66 lbs), sex (male intact, male neutered, female intact, and female spayed), vaccination status (no, yes), other household pets (no, yes), current medication status (no, yes), duration of clinical signs related to the current compliant (0–6 hrs, 7–12 hrs, 13–18 hrs, 19–24 hrs, 25–48 hrs, 49–72 hrs, >72 hrs), diarrhea (no, yes), vomiting (no, yes), lethargy (no, yes), anorexia (no, yes), abdominal distention (no, yes), past medical history (no history, history unrelated to GI, history related to GI), and other clinical signs (no, yes history unrelated to GI, yes history related to GI). Examples of other clinical signs related to the GI include drooling, weight loss, pain, licking, and eating grass. The outcome of the telehealth visit regarding the recommendation for emergency referral (no, yes) was also recorded. Data analysisData were analyzed as a retrospective cohort study with referral to an ER clinic as the binary outcome variable of interest. All other data were considered independent variables and were coded as categorical, ordinal, or binary as appropriate. Summary descriptive statistics include frequency counts, percentages, odds ratios, means, medians, SDs, and quartiles. The primary statistical objective was to determine which variables were significantly associated with referral to the emergency facility. The chi-square test for rx2 contingency tables was used to test for individual associations. Multiple logistic regression with backward elimination variable selection, based on Akaike’s information criterion (AIC), was used to determine which features were jointly significantly associated with ER visit recommendation. Logistic regression was also used to analyze specific two-way interactions in the context of post hoc exploratory analyses. A result was considered statistically significant if p<0.05. All data were analyzed using R statistical software (Version 4.3.2) (Rstudio, 2022). Ethical approvalNot needed for this study. ResultsStudy populationA total of 11,109 records representing 11,109 synchronous video-based teletriage sessions conducted by 47 veterinarians were reviewed, of which 1,575 were found to meet the inclusion criteria. The median weight of the 1,575 dogs included in the study was 34 lbs [IQR 15–60lbs; mean 40 ± 29lbs; range 1–190lbs]. The median age of all dogs was 3.5 years [IQR 1–8 years; mean 4.7 ± 3.9 years; range 0–16 years]. Table 1 illustrates the dog distributions across the other categorical variables recorded. The most common clinical complaint was vomiting (62%; 977/1575), followed by diarrhea (43%; 670/1575). Most dogs had been experiencing acute clinical signs related to the GI tract for six hours or less (40%; 635/1575). Overall, 23% of dogs (360/1575) were recommended to be referred to an emergency veterinary facility. Table 1. Univariable analysis of factors associated with recommendation for in-person emergency evaluation for dogs presenting to a teletriage service for GI signs. Number (N) and percentage (%) are given. Significance is set a p < 0.05; OR with a 95% CI are provided for all variables identified as significant.
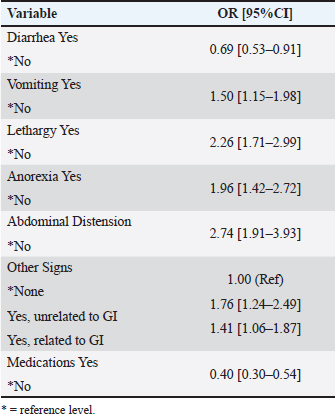
Factors associated with ER referralUnivariable analyses, based on the chi-square test, revealed that the following eight variables were associated with ER referral rate: age group (p < 0.011), diarrhea (p < 0.001), vomiting (p < 0.002), lethargy (p < 0.0001), anorexia (p < 0.0001), abdominal distention (p < 0.0001), the presence of other clinical signs (p < 0.0001), and medications (p < 0.0001). With the exception of age, diarrhea, and medications, the presence of a factor was associated with an increased risk of emergency facility referral. However, the presence of diarrhea or medications was associated with a decreased risk of emergency facility referral. When these eight variables were entered in a multivariable logistic regression model, subject to backward variable selection, seven of these variables (age group was eliminated) were independently and significantly associated with ER referral (Table 2): diarrhea (OR=0.69 [0.53–0.91], vomiting (OR=1.50, 95%CI=[1.15–1.98]), lethargy (OR=2.26 (1.71–2.99), anorexia (OR=1.96 [1,42–2.72]), abdominal distention (OR=2.74 [1.91–3.93]), the presence of other clinical signs (OR=1.76 [1.24–2.49] for signs unrelated to GI and OR=1.41 [1.06–1.87] for signs related to GI), and medications (OR=0.40 [0.30–0.54]) when compared to the reference category of “No” or “None.” Table 2. Results of multivariate logistic regression (OR and 95% CI) after selection of backward variables.
Abdominal distention and lethargy were associated with the greatest increase in the odds of being recommended for emergency referral (174% and 126%, respectively). Vomiting, as the most commonly identified clinical sign, was associated with a 50% greater odds of being recommended for referral. Diarrhea (31% lower odds), a current history of being on medications (60% lower odds), and being over 8 years of age (19% lower odds) were negatively associated with referral to an emergency facility (Table 2). Multivariate analysisA multivariable logistic regression model using all 16 factors as independent variables and recommendation for emergency referral as the binary outcome revealed significant positive associations between referral and having a previous medical history unrelated to the GI (p=0.013), vomiting (p=0.002), lethargy (p < 0.0001), anorexia (p < 0.0001), abdominal distention (p < 0.0001), and other clinical signs both related (p=0.005) and unrelated (p=0.003) to the GI. The presence of diarrhea (p=0.028), a history of vaccination (p=0.03), and a current history of medication (p < 0.0001) were significantly negatively associated with the recommendation for emergency referral. Backward selection using AIC reduced the model to the following five positively associated variables: vomiting (p=0.003), lethargy (p < 0.0001), anorexia (p=0.0001), other clinical signs both related (p=0.014) and unrelated (p < 0.001) to the GI, and abdominal distention (p < 0.0001); and one negatively associated variable: current history of receiving medication (p < 0.0001). As vomiting was the most common presenting sign, further exploratory analysis was conducted to evaluate for possible interactions that would be associated with referral to the emergency facility. Exploratory analysis revealed significant interactions between vomiting and other GI tract-related clinical signs (p=0.014). In the subgroup of dogs that had no vomiting, there was no significant difference in the risk of referral to the ER among the three categories of other clinical signs (no signs, signs related and unrelated to GI; p=0.22). Vomiting dogs with additional clinical signs, both related (28.2%) and unrelated (35.3%) to the GI tract, had a significantly higher ER referral rate than those without other clinical signs (19.2%; p=0.0001). DiscussionThis retrospective review of a large sample of dogs presented to a veterinary teletriage service demonstrated a low referral rate of 23% for in-person emergency care for dogs presenting with GI symptoms. Televeterinarians were able to collect clinically relevant information from consultation with animal owners and caretakers, and through real-time video evaluation of the patient, were able to consider patient status and provide triage regarding the need for referral versus advice and monitoring. This did not extend into the realm of diagnosis or treatment requiring a prescription. This mechanism of providing triage and advice to a broad population of dogs and clients holds tremendous promise for maximizing the utility of the veterinary ER workforce and expanding access to care options that are reliable and maintain a high quality of practice, as supported by the human literature (Gonçalves and Shah, 2024; Farzandipour et al., 2024). In the provision of teleadvice through teletriage in this study, there was no requirement for establishing a VCPR. Here, the DVM was able to collect important and clinically relevant information about the patient, such as lethargy or anorexia, and other information that would be otherwise difficult for clients to assess, such as abdominal distention. The use of real-time videoconferencing enabled the DVM, who is trained to perform teletriage, to observe the patient and instruct the owner to perform certain manipulations or examinations to further evaluate symptoms. For example, during a real-time live video, the veterinarian observes that the normally tucked-in abdomen is replaced by a distended abdomen, as evidenced by a combination of the owner’s historic account and manual pressure placed by the pet owner on the ventral abdomen of the pet under the real-time direction and supervision of the televeterinarian. In a study surveying the experiences of veterinarians with telehealth, 1- and 2-way video were the least reported telecommunication platforms utilized (Watson et al., 2019), indicating the unique nature of this approach. Although other platforms have been developed since that study, at the time of this publication, such resources lack both published data and synchronous access for pet owners to experienced veterinarians on a 24/7 basis for the sole purpose of teletriage and teleadvice (Smiley, 2022). Nevertheless, no firm diagnosis was rendered on the basis of these virtual findings, and no prescriptions were given, avoiding over-interpretation of such findings and eschewing the need for VCPR. A human study has shown the effectiveness of teletriage, where low-risk patients were triaged, and high-risk patients were directed to a face-to-face appointment (Gonçalves and Shah, 2024). Overall, clients and patients received prompt veterinary care and were able to obtain valuable triage and advice, irrespective of the emergency status of the pet’s condition. Ultimately, only 360 of 1,575 dogs (23%) were recommended for in-person emergency evaluation following teletriage consultation. While it is unknown what number of those originally presenting would have otherwise visited an ER in the absence of teletriage accessibility, the ability of experienced veterinarians to utilize the information at hand to aid in differentiating those dogs in need of immediate in-person emergency services due to GI symptoms from those not in need (e.g., teletriage) represents an opportunity to streamline the most appropriate cases to the ER and, in turn, to maximize the veterinary ER workforce (Donahue, 2022). This is supported by a study in human medicine where tele-triage interventions during COVID-19 reduced unnecessary ER visits by up to 22.2% (Farzandipour et al., 2024). Burnout is a major factor contributing to the intent to leave practice among ER veterinarians, and workload may contribute directly to such feelings (Hayes et al., 2020; Booth et al., 2021; Holowaychuk and Lamb, 2023). In most veterinary clinics, clients are pre-screened by a client service representative, whereas in others, a veterinary technician (or equivalent) may be available, although unreliable due to given workloads and staffing challenges. This approach does not provide the same medical quality as DVM triage. The use of an attending clinician or an intern may be helpful, although availability is inconsistent and is not the most effective use of in-house time. Improving the case selection of patients who present to an ER by using veterinarians to triage patients through telehealth could improve workflow, the quality of the ER work environment, and possibly even the retention of ER veterinarians and staff. It is unknown what proportion of the dogs reviewed here accessed services via which pathway; however, anecdotally, many clients seeking teletriage/teleadvice services do so because they cannot access a veterinarian due to location or availability constraints. While over 90% of dog owners report using veterinary services, only 40% of them report doing so annually (Bir et al., 2020). In 2022, the average total annual spending on veterinary care reported by dog owners was $367 (AVMA, 2022); a single visit to the teletriage platform described here costs markedly less than an ER hospital visit, which might range widely from $150 to multiple thousands of dollars, even for basic examination and diagnostics (MetLife Pet Insurance, 2024). Through teletriage, telehealth can provide clients with access to emergent veterinary care along a spectrum of economic, geographic, and physical constraints to obtain a quality level of veterinary care for their pet. The most common presenting complaint among the observed population of dogs was vomiting, which is similar to what has been shown elsewhere (Parr and Otto, 2013; Saito and Rhoads, 2021; Holzmann et al., 2023). The presence of vomiting resulted in a 50% higher odds of recommendation for in-person ER evaluation, and vomiting was ultimately retained in the final multivariable model of factors associated with referral. Given the prevalence of this sign, interactions with other variables were examined through exploratory analysis, demonstrating that the presence of vomiting alongside other clinical signs, both related and unrelated to the GI tract, increased the risk for ER referral. These findings that the clinical sign of “vomiting” increases the chance of presenting at the ER are also consistent with a recent study where 66% of dogs that presented to an ER with vomiting were categorized as complicated vomiting, as they required additional investigation, surgery, or support that exceeded simple symptomatic treatment (Hubbard et al., 2007). Previous studies have also shown that vomiting is a common cause of canine presentation to the ER (Parr and Otto, 2013; Saito and Rhoads, 2021). Lethargy and abdominal distention were associated with 174% and 126% increases, respectively, in the odds of referral to the ER and were also factors ultimately retained in the final multivariate logistic model. It is unsurprising that these symptoms were associated with increased referral probabilities, as lethargy and abdominal distention typically represent a severe disease state such as obstruction, hemoperitoneum, peritoneal effusion, or other advanced or critical pathologies. The identification of these severe findings as having such high odds in predicting an in-person ER examination supports the use of this teletriage evaluation platform for effectively identifying at-risk patients. In general, the above findings, derived from a large sample of dogs, diverse in signalment and geographic distribution throughout the US, evaluated by a variety of experienced veterinarians who do not originate from the same hospital or even location, may provide insights that can be used outside of a telemedicine setting to help ER clinics and veterinary hospitals more effectively triage their own incoming cases in emergent settings. In contrast, diarrhea, currently being on medication, and a history of vaccination were all negatively associated with a recommendation for in-person ER evaluation. Diarrhea has been described as a common and often self-limiting complaint that does not consistently rise to the level of veterinary intervention (Hubbard et al., 2007). While receiving medications and a history of vaccination were independently associated with a lower odds of referral to the ER, only a current history of receiving medication was retained in the final multivariate model. These two factors appear to exert a protective effect on dogs with regard to emergent GI disease. Such an effect could be mediated directly; for example, dogs who have received a parvovirus vaccination are at less risk of developing potentially life-threatening parvoviral gastroenteritis (Wang et al., 2024). Alternatively, this effect could be indirectly moderated; for example, dogs who are currently on medication (which may include prescription preventatives) may be those routinely receiving veterinary care and may therefore be less at risk for disease compared with another population that is not routinely seeing a veterinarian. Such an established medical intervention has the added potential to be modified virtually by a veterinarian. Regardless of the reasons behind why diarrhea, medication status, and vaccine history resulted in a lower likelihood of ER referral, a teletriage veterinarian can collect and synthesize important information to provide a tailored veterinary recommendation to each individual patient. Despite the findings and usefulness of services described here, this study has some limitations. The validity of the in-person ER referral recommendations made by teletriage veterinarians in this study was first considered. In other words, how many of the 360 patients referred to the ER truly required emergent veterinary care, and how many of the 1,215 patients who were not recommended immediate in-person evaluation did? No follow-up was performed on the dogs described in this study to determine whether they went to the ER, obtained a diagnosis, or were followed up with their regular provider to validate the findings or advice provided by the teletriage DVM. Additionally, despite the veterinarians involved being experienced clinicians, the information gathered and the determinations made regarding each case were based on the accuracy of medical records written by the individual televeterinarians. Regardless, no diagnosis was made during the teletriage exam, which could later be validated through an in-person exam. Furthermore, when an animal arrives at a veterinary clinic asking for emergency treatment, no standardized criteria are used to confirm the existence of a true emergency exists. Beyond the AVMA definition of emergency care of “necessary to save life or relieve suffering,” most animals presenting on an emergency basis will receive an examination and diagnosis, and many will receive therapy either in the form of supportive care or as an intervention. Therefore, the determination of anything other than a life-threatening condition as emergent is, at best, subjective, suggesting that there is no true validation that can be applied to teleadvice. Nevertheless, future studies evaluating the correlation of the telehealth assessment with case outcomes are needed. The second limitation is that the patient population may not represent a typical case population that might be expected to present to a veterinary clinic. It is possible that at least some of the clients leveraging teletriage and teleadvice services struggle with access to care or do not routinely use veterinary services for other reasons. Therefore, the dogs described here may represent some differences from those typically seen in a veterinary hospital or ER facility. Alternatively, dogs exhibiting more severe signs may be less likely to utilize a teletriage service and instead go directly to an in-person emergency service, creating a somewhat biased sample population in this study. Despite possible data weaknesses, the large size of the population observed here, and the utility of the advice services provided, remain relevant. To the best of the author’s knowledge, this is the first publication that reports the successful assessment and triage of a large number of dogs with clinical signs consistent with acute and chronic gastroenteropathies through a novel synchronous veterinary teletriage and teleadvice video platform. The usefulness and versatility of such a platform is apparent, as this critical service can provide high-quality advice in the absence of a VCPR and can support the veterinary workforce, as well as a client and patient population with a range of economic and geographic requirements. The popularity of the telehealth modality is anticipated to continue to increase for pets with various medical and traumatic conditions, as well as amongst pet owners, wildlife rescue personnel, and the veterinary community. In addition to further research on a larger range of species and pathologies, more work by veterinarians is needed to continue to establish guidelines for the execution of high-quality telehealth and its subcategories. AcknowledgmentsThe authors declare that there are no acknowledgments. FundingThis research received no specific grant. Authors’ contributionsShadi J. Ireifej: data collection, literature search, initial manuscript creation, subsequent manuscript edits, manuscript finalization, and submission. Samantha L. Morello: manuscript edits, statistical analysis. Marty Lesser: statistical analysis. Conflict of interestThe authors declare that there is no conflict of interest. Data availabilityThe data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. ReferencesAmerican Kennel Club. Everything we do, we do for dogs. Available via www.akc.org (Accessed 30th April 30, 2024). AVMA. 2022. AVMA pet ownership and demographic sourcebook American Veterinary Medical Association. AVMA, Schaumburg, IL. AVMA. AVMA guidelines for telehealth use in veterinary practice. Available via https://www.avma.org/sites/default/files/2021-01/AVMA-Veterinary-Telehealth-Guidelines.pdf (Accessed 30th April 30, 2024). AVMA. Definitions of telehealth; Talking about telehealth. Available via https://www.avma.org/sites/default/files/2021-02/Telehealth-definitions-AVMA.pdf (Accessed 30th April 30, 2024). AVMA. Principles of veterinary medical ethics of the AVMA. Available via https://www.avma.org/resources-tools/avma-policies/principles-veterinary-medical-ethics-avma (Accessed 30th April 30, 2024). Bain, B., Hanson, C., Ouedraogo, F. and Salois, M. 2019. AVMA Report on the economic state of the veterinary profession. Washington, DC: American Veterinary Medical Association. Booth, M., Rishniw, M. and Kogan, L.R. 2021. The shortage of veterinarians in emergency practice: a survey and analysis. J. Vet. Emerg. Crit. Care 31(3), 295–305. Cushing, M. 2022. What are telemedicine, telehealth, and teletriage?. Vet. Clin. North Am. Small Anim. Pract. 52(5), 1069–1080. Donahue, K. 2022. Teletriage: remote advice provides better care. Vet. Clin. North Am. Small Anim. Pract. 52(5), 1081–1086. Farzandipour, M., Nabovati, E. and Sharif, R. 2024. Effectiveness of tele-triage during the COVID-19 pandemic: a systematic review and narrative synthesis. J. Telemed. Telecare. 30(9), 1367–1375. Finstad, J.B., Rozanski, E.A. and Cooper, E.S. 2023. Association between the COVID-19 pandemic and the prevalence of cats presenting with urethral obstruction at two university veterinary emergency rooms in Japan. J. Feline. Med. Surg. 25(2), e007. Gonçalves, R.B. and Shah, M. 2024. Patient satisfaction with a skin cancer tele-triage system. Indian J. Dermatol. 69(4), 352–353. Hayes, G.M., LaLonde-Paul, D.F., Perret, J.L., Steele, A., McConkey, M., Lane, W.G., Kopp, R.J., Stone, H.K., Miller, M. and Jones-Bitton, A. 2020. Burnout syndrome and job-related risk factors in veterinary technicians in specialty teaching hospitals: a multicenter cross-sectional study. J. Vet. Emerg. Crit. Care. 30(1), 18–27. Holowaychuk, M.K. and Lamb, K.E. 2023. Symptoms of burnout and workplace satisfaction among veterinary emergency care providers. J. Vet. Emerg. Crit. Care 33(2), 180–191. Holzmann, B., Werner, M., Unterer, S. and Dörfelt, R. 2023. Utility of diagnostic tests in dogs with vomiting who presented to an internal medicine emergency service. Front. Vet. Sci. 10, 1063080. Hubbard, K., Skelly, B.J., McKelvie, J. and Wood, J.L.N. 2007. Risk of vomiting and diarrhea in dogs. Veter. Rec. 161, 755–757. Ireifej, S. and Krol, J. 2023. Case studies of 15 novel species successfully aided by a veterinary teletriage service. Front. Vet. Sci. 5(10), 1225724. MetLife Pet Insurance. 2024. How much does an emergency visit cost? https://www.metlifepetinsurance.com/blog/pet-health/emergency-vet-cost (Accessed 30th April 30, 2024). Parr, J.R. and Otto, C.M. 2013. Emergency visits and occupational hazards in German Shepherd police dogs (2008-2010). J. Vet. Emerg. Crit. Care. 6, 591–597. R Core Team. 2022. R: a language and environment for statistical computation. R Foundation for Statistical Computing, Vienna, Austria. Available via https://www. R-project.org/ (Accessed 24th February 24, 2024). RStudio: integrated development environment for R. Posit Software, 2022. (Accessed 24th February, 2024). Ruxin, T., Feldmeier, M., Addo, N. and Hsia, R.Y. 2023. Trends by acuity for emergency department visits and hospital Admissions in California, 2012 to 2022. JAMA. Netw. Open. 6(12), e2348053. Saito, E.K. and Rhoads, C. 2021. Emergency visits to primary care veterinary hospitals. Vet. Focus Roy. Canin. 25(3), 18-19. Available via https://vetfocus.royalcanin.com/en/scientific/emergency-visits-to-primary-care-veterinary-hospitals Smiley. 2022. Asynchronous veterinary telemedicine. North Am. Small Anim. Pract. 52(5), 1135–1140. Wang, Z., Shi, P., Wang, S., Lin, Z., Wang, Z., Zhang, C., Zhao, L., Suolang, S., Zou, J. and Zhou, H. 2024. Generation of canine neutralizing antibodies against canine parvovirus using single B-cell antibody technology. Arch. Virol. 169(11), 225. Watson, K., Wells, J., Sharma, M., Robertson, S., Dascanio, J., Johnson, J.W., Davis, R.E. and Nahar, V.K. 2019. A survey of knowledge and use of telehealth among veterinarians. BMC Vet. Res. 15(1), 474. Wayne, A.S. and Rozanski, E.A. 2020. Weekly surveys to catalog the response by emergency veterinary hospitals during the COVID-19 pandemic. J. Vet. Emerg. Crit. Care. 30(4), 493–497. | ||
| How to Cite this Article |
| Pubmed Style Ireifej SJ, Morello SL, Lesser M. Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. Open Vet. J.. 2026; 16(1): 363-371. doi:10.5455/OVJ.2026.v16.i1.33 Web Style Ireifej SJ, Morello SL, Lesser M. Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. https://www.openveterinaryjournal.com/?mno=272613 [Access: June 26, 2026]. doi:10.5455/OVJ.2026.v16.i1.33 AMA (American Medical Association) Style Ireifej SJ, Morello SL, Lesser M. Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. Open Vet. J.. 2026; 16(1): 363-371. doi:10.5455/OVJ.2026.v16.i1.33 Vancouver/ICMJE Style Ireifej SJ, Morello SL, Lesser M. Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. Open Vet. J.. (2026), [cited June 26, 2026]; 16(1): 363-371. doi:10.5455/OVJ.2026.v16.i1.33 Harvard Style Ireifej, S. J., Morello, . S. L. & Lesser, . M. (2026) Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. Open Vet. J., 16 (1), 363-371. doi:10.5455/OVJ.2026.v16.i1.33 Turabian Style Ireifej, Shadi J., Samantha L. Morello, and Marty Lesser. 2026. Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. Open Veterinary Journal, 16 (1), 363-371. doi:10.5455/OVJ.2026.v16.i1.33 Chicago Style Ireifej, Shadi J., Samantha L. Morello, and Marty Lesser. "Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs." Open Veterinary Journal 16 (2026), 363-371. doi:10.5455/OVJ.2026.v16.i1.33 MLA (The Modern Language Association) Style Ireifej, Shadi J., Samantha L. Morello, and Marty Lesser. "Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs." Open Veterinary Journal 16.1 (2026), 363-371. Print. doi:10.5455/OVJ.2026.v16.i1.33 APA (American Psychological Association) Style Ireifej, S. J., Morello, . S. L. & Lesser, . M. (2026) Retrospective analysis of teletriage and teleadvice administered to 1,575 dogs with gastrointestinal signs. Open Veterinary Journal, 16 (1), 363-371. doi:10.5455/OVJ.2026.v16.i1.33 |

