




| Case Report | ||
Open Vet. J.. 2026; 16(1): 731-738 Open Veterinary Journal, (2026), Vol. 16(1): 731-738 Case Report Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findingsKübra Yağlı1*, Görkem Ekebaş1, Gökçen Perk2, Gültekin Atalan2 and Latife Çakır Bayram11Department of Pathology, Faculty of Veterinary Medicine, Erciyes University, Kayseri, Turkey 2Department of Surgery, Faculty of Veterinary Medicine, Erciyes University, Kayseri, Turkey *Corresponding Author: Kübra Yağlı. Department of Pathology, Faculty of Veterinary Medicine, Erciyes University, Kayseri, Türkiye 38039, Turkey. E-mail: kubrayagli [at] erciyes.edu.tr; kubra.ygli [at] gmail.com Submitted: 07/08/2025 Received: 19/11/2025 Accepted: 03/12/2025 Published: 31/01/2026 © 2025 Open Veterinary Journal
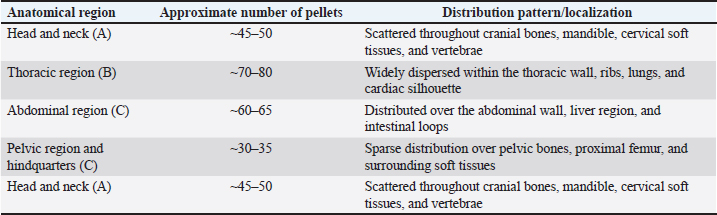
AbstractBackground: Although firearm-related injuries are relatively uncommon in veterinary forensic pathology, they constitute an important cause of animal traumatic death. Accurate forensic evaluation of such cases necessitates an integrative, multidisciplinary approach to determine the cause and manner of death. Case description: This report presents the forensic investigation of a 5-year-old male Cane Corso dog found dead with no prior clinical signs. Necropsy revealed multiple pellet entry wounds on the skin and soft tissues. Radiographic and gross pathological examination demonstrated widespread pellet distribution in the thoracic and abdominal cavities. Histopathological analysis confirmed multi-organ damage, including hemorrhage, necrosis, and tissue disruption in the heart, lungs, and liver. Although the firearm was not recovered, a close-range discharge was indicated by ballistic analysis. Conclusion: The manner of death was determined to be multi-organ trauma resulting from close-range shotgun pellet penetration. This case highlights the forensic significance of penetrating firearm injuries in veterinary pathology and emphasizes the need for a multidisciplinary approach in investigating such cases. Keywords: Forensic veterinary pathology, Gunshot wound, Necropsy, Pellet injury, Wound ballistics. IntroductionRecent studies and empirical observations have reported a phenomenal rise in the use of guns not only on wildlife but also on domesticated animals and livestock. Guns are utilized daily in the offenses of unjustifiable killing, theft, and animal cruelty (Barach et al., 1986; Alcigir et al., 2014; Aksoy et al., 2013). The accidental or intentional shooting of wild and domestic mammals is a frequent issue in veterinary forensic pathology, usually with lethal consequences (Cooper and Cooper, 2008). In such instances, more than one category of firearm, such as handguns, shotguns, and pump action rifles, and penetrating injuries are inflicted that result in severe tissue and internal organ damage. In animal models, these types of injuries can manifest with clinical signs of respiratory distress, lethargy, lameness, pneumothorax, internal hemorrhage, and fractures, and in their more severe forms, they frequently result in death (Cooper and Cooper, 2008; Kneubuehl et al., 2011; Grela et al., 2021). Although firearm-related injuries account for a relatively small proportion of clinical and necropsy cases in veterinary practice, their occurrence in domestic animals, particularly dogs, has been confirmed in several studies. In a retrospective survey of dogs with radiographically confirmed projectiles, gunshot injuries were found to represent zero. Seventy-six of all cases (Capak et al., 2016). Similarly, in a large-scale forensic investigation involving multiple species, firearms were implicated in more than half of the examined cases, with dogs comprising approximately six. 6.7% of the victims (Khankhasykov et al., 2024). Recent reports have also highlighted an increasing trend of firearm injuries in companion animals, many of which are associated with deliberate cruelty or unlawful killing (Olsen et al., 2014; Crofts et al., 2023). Beyond their clinical significance, such cases hold considerable forensic value, as radiographic and pathological findings can serve as crucial evidence for differentiating antemortem from postmortem injuries, reconstructing shooting distance and direction, and establishing the cause of death. The present case adds to the limited veterinary forensic literature by documenting a fatal cardiac tamponade secondary to multiple shotgun pellet impacts, in which both penetrating and concussive blast-type mechanisms were implicated as features rarely described in previous reports, such as Bradley-Siemens and Brower (2016) and Piegari et al. (2024). The primary function of veterinary forensic pathology is to assist legal institutions with thorough investigation results backed by empirical evidence (Pavletic and Trout, 2006). These findings are essential for elucidating what happened in the case, revealing factual information, and facilitating a just legal process (Fox et al., 2020). Pathological data derived through necropsy plays a central role in verifying the accuracy of forensic results. The purpose of such autopsies is not only to establish the manner of death but also to identify and record physical evidence, including but not limited to bullets, pellets, or shell fragments. Recording entry wounds and paths of injuries on the body (Fox et al., 2020). Case DetailsA 5-year-old male Cane Corso was found dead in the garden of a single-family house. Based on the presented history, the dog did not present any clinical signs of disease before death. Although the owner could not establish the definitive cause of death, there was a strong suspicion that the dog could have been deliberately harmed. Accordingly, a judicial investigation was launched, and the case was sent to the Department of Pathology within the Faculty of Veterinary Medicine in Erciyes University for identification of the cause of death in accordance with the instructions of the Public Prosecutor’s Office. A whole-body radiographic examination was performed in the latero-lateral position before necropsy using a digital radiography system, Ajex Meditech, model BLD 150AJ, in accordance with standard forensic imaging protocols. Exposures were taken at a tube voltage of 80 kV and current time settings of 25 mAs. The radiographs revealed multiple radiopaque foreign-body densities in the cervical, thoracic, and abdominal regions consistent with shotgun pellets. On gross examination, mild soot deposition, gunpowder residue, and parchment-like epidermal changes were observed around the pellet entry wounds, limited to the cervical region. The restriction of these findings to this localized area suggests that the first discharge may have been fired from a closer range toward the neck. However, the absence of such close-range indicators in other anatomical regions, together with the wide distribution of pellets throughout the body, supports the interpretation that the shots were generally fired from a long distance and in rapid succession. The uniform distribution pattern of the wounds and their smooth, rounded margins further reinforce this assessment, indicating that the lesions most likely resulted from multiple long-range discharges fired in short intervals (Table 1). Table 1. Anatomical localization and shotgun pellet density pattern.
Subsequently, a comprehensive systemic necropsy was conducted following the guidelines for veterinary forensic necropsy. Tissue samples were collected from the brain, lungs, heart, liver, kidneys, intestines, and spleen and fixed in 10% neutral buffered formalin. After routine tissue processing, the samples were paraffin-embedded, sectioned at 4–5 µm thickness, and stained with hematoxylin and eosin (H&E). A light microscope (Olympus CX31, Tokyo, Japan) was used for histopathological evaluation. Thirty-six pellets (weight range: 0.172–0.197 g; diameter range: 2–3 mm) were obtained during necropsy and reserved for submission to the judiciary (Fig. 1). Multi-organ damage secondary to penetrating pellet trauma resulting in hypovolemic and cardiogenic shock due to cardiac tamponade was determined as the manner of death.
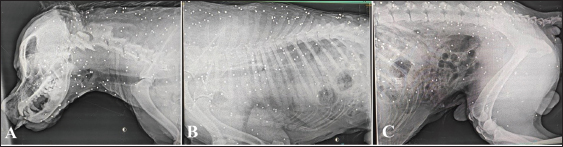
Fig. 1. Shotgun pellets were retrieved postmortem from various anatomical regions and collected in a sterile Petri dish. The metallic appearance and uniform spherical morphology are consistent with those of typical lead-based birdshot ammunition. Lateral position radiographs revealed numerous radiopaque metallic densities of shotgun pellets in different organs and tissues. Pellet concentrations were particularly pronounced in the head (Fig. 2A), thoracic (Fig. 2B), and abdominal regions (Fig. 2C), whereas a relatively sparse pattern was observed in the right hind limb. Increased opacity and lack of sharpness of the costal margin were observed in the thoracic region, which may suggest the presence of hemothorax.
Fig. 2. Laterolateral radiographic views of the dog showing metal dense opacities in the head (A), thoracic (B), and abdominal (C) regions corresponding to shotgun pellets. The distribution of pellets appears to be more widespread in the thoracic and abdominal areas. During necropsy, postmortem rigidity was lost. Gross examination revealed multiple circular shotgun entrance wounds (0.5–1 cm in diameter) with smooth borders around the patient’s body. No abnormalities or traumatic lesions were observed during the external examination and in situ inspection of the dog (Fig. 3). However, a detailed examination of the entire body and limbs revealed multiple entrance wounds to the shotgun pellet. The entrance wounds were located on the skin of the head and neck regions (regio oralis, buccalis, temporalis, and colli dorsalis) (Fig. 4), trunk (regio scapularis, costalis, and xiphoidea) (Fig. 5), and right hind limb (regio femoralis, tibialis, and phalanges proximalis). Following skin removal and disarticulation of the limbs, embedded pellets were discovered in the parotid area, within the latissimus dorsi muscle of the scapular area, along the path of the femoral artery of the femoral area, and surrounding the common carotid artery and jugular vein of the submandibular and ventral cervical areas.
Fig. 3. The general appearance of the dog before necropsy.
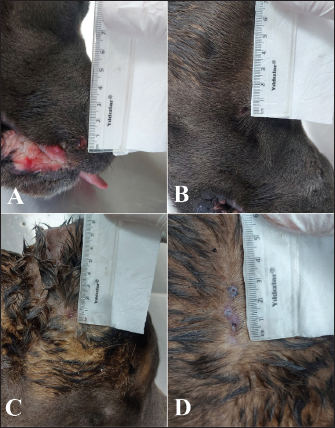
Fig. 4. Pellet entry wounds observed in the head and neck regions of the dog. (A) Rounded entry wound with regular margins located in the left labial region (regio labialis sinistra); (B) small, single entry wound with mild surrounding hemorrhage in the right temporal region (regio temporalis dextra); (C) pellet entry sites in the occipital region (regio occipitalis); (D) two adjacent, small entry wounds with smooth edges and mild ecchymosis on the dorsolateral neck region (regio colli dorsolateralis).
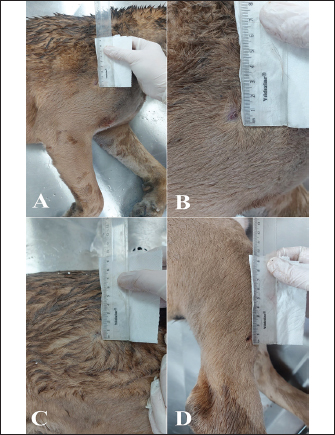
Fig. 5. Pellet entry wounds observed in the dog’s trunk and limb regions. (A) Mildly ecchymotic pellet entry hole located cranial to the scapula in the right cranial thoracic region; (B) small, well defined entry wound situated along the anterior margin of the right scapular area, near the proximal forelimb; (C) smooth-edged pellet entry sites with minimal hemorrhagic halo on the right dorsal thoracic area, adjacent to the thoracic vertebrae; (D) small, rounded, well entry wound located on the distal femoral region of the right hind limb. The absence of hemorrhage or coagulum in the immediate surroundings of the implanted pellets was of specific interest, other than in the jugular vein and the xiphoid area. However, the jugular vein did have signs of compromise, and the surrounding soft tissue was completely coated with coagulated blood, a very significant finding. Likewise, extensive subcutaneous hemorrhage was observed in the xiphoid area. Macroscopic examination of the heart revealed an extensive collection of clotted blood within the pericardial cavity (Fig. 6A). The ventral aspect of the left ventricular wall, near the midline, had a well-demarcated and well-marginated penetration defect measuring approximately 0.5 cm (Fig. 6B). The right ventricular wall also exhibited a small exit wound near the apex cordis (Fig. 6C).
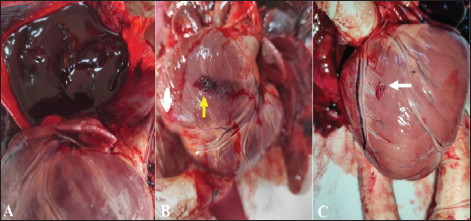
Fig. 6. (A) Accumulation of clotted blood in the pericardial sac; (B, C) entry wound of a shotgun pellet in the left ventricle (yellow arrow) and exit wound in the right ventricle (white arrow). The lungs were collapsed, and two shotgun pellets were identified in the right lung cranial and caudal lobes (Fig. 7A). Blood clots were present within the trachea, bronchi, and bronchioles.
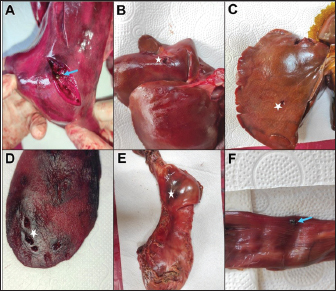
Fig. 7. (A) A metallic, shiny shotgun pellet localized within the pulmonary parenchyma of the right lung lobe (blue arrow); (B–E) Pellet entry holes (white asterisks) observed in the liver lobes, spleen, and stomach; (F) A metallic shiny pellet dissected from the subserosa of the rectum (blue arrow). In the abdominal cavity, blood clots were found on the omentum majus, and one pellet penetrated the diaphragm. Three pellet wounds were found in the liver (Fig. 7B and C). In the medial aspect of the right kidney, close to the hilus renalis at the facies sinister, one pellet defect measuring 0.5–1 cm was observed. A blood clot measuring 3 × 5 × 8 cm was present anterior to the hilus renalis, through which the renal artery and vein entered. Some circular perforations (2–4 mm in diameter) were observed in the spleen on its parietal surface Figure 7D. Pellet entry wounds were observed on the serosal surface of the stomach, particularly along the curvatura major, and focal mucosal hemorrhage was observed in the pyloric region (Fig. 7E). One pellet was identified in the subserosal layer of the rectum with some bleeding around it (Fig. 7F). Microscopic findings included multifocal hemorrhage and loss of myocardial fiber integrity around the left ventricle (Fig. 8A and D). The lungs were emphysematous with hemorrhage in the bronchi, bronchioles, and alveolar lumens (Fig. 8E and H). The kidneys exhibited diffuse interstitial hemorrhage throughout the cortex, medulla, and perirenal pelvis (Fig. 8I and L).
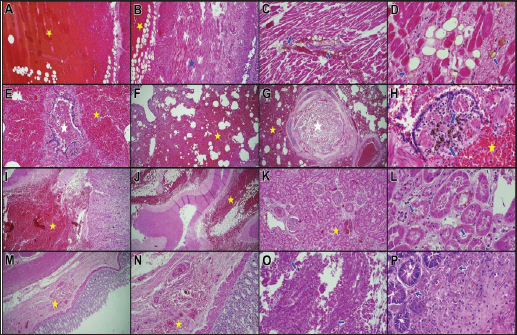
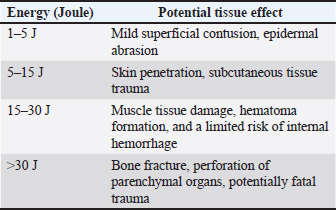
Fig. 8. (A, B) Extensive hemorrhagic areas (yellow asterisks) and disruption/loss of myocardial fibers (blue asterisks); (C, D) Yellowish amorphous aggregates associated with shotgun pellets (blue arrows) accompanied by myocardial hemorrhage; (E–G) Widespread interalveolar hemorrhage in the lung (yellow asterisks), and erythrocyte clusters in the bronchial and bronchiolar lumens (white asterisks); (H) Yellowish amorphous aggregates in the bronchiolar lumen associated with shotgun pellet injury (blue arrow); (I–K) Diffuse hemorrhagic areas in the renal pelvis and erythrocyte clusters in the intertubular areas of the kidney (yellow asterisks); (L) Yellowish granular material deposits in the renal tubular epithelium due to pellet-related trauma (blue asterisk); (M, N) Hemorrhagic areas in the submucosa of the intestine (yellow asterisks); (O, P) Yellowish amorphous aggregates within the intestinal lumen and submucosa related to shotgun pellet injury. Scale bars: 200 µm for A–C, F, I–K, M, N; 100 µm for D, E, G, H, L, O, P. Stain: Hematoxylin and eosin. The same hemorrhages were also observed in the small intestine submucosal layers. Notably, a yellowish granular substance was deposited in the subserosal tissue of the heart, lungs, kidneys, and intestines (Fig. 8M–P). Histopathological examination was performed on all major organs; however, only those showing direct pellet impact and characteristic lesions such as severe hemorrhage, structural disruption, and yellowish granular deposits were presented in the microscopic figures. The kinetic energy E ½ m v² of the shotgun pellets was calculated assuming an average pellet velocity of 375 ms, which falls within the typical muzzle velocity range reported for standard 12-gauge shotgun ammunition (350–400 m/s) (Ordog et al., 1984; Kneubuehl et al., 2011; Bradley-Siemens and Brower, 2016). This estimated value was used to approximate the energy transferred to the tissues. The calculation is theoretical and may not account for the physical and biological factors influencing energy dissipation. The findings cite the theoretical energy transported by one pellet. The energy is sufficient to produce penetrating injuries in superficial tissues. However, several external and biological factors, such as air resistance, tissue density, and pellet deformation, can significantly reduce the effective kinetic energy reaching deeper organs. Therefore, the calculated energy values represent an approximation of the initial impact rather than the true energy transferred within the tissues. However, in the current scenario, despite the presence of perforating scalp wounds, the pellets failed to penetrate the cranial bones, implying that a high proportion of the energy was substantially dissipated in the skin and subcutaneous tissues (Table 2). Table 2. Definition and significance of the “Joule” unit in veterinary forensic pathology.
DiscussionsThe heart is an important organ that can be significantly impacted by firearm injuries, both penetrating and indirect. These types of injuries are usually fatal (Barach et al., 1986; Cooper and Ryan, 1990; Pavletic and Trout, 2006; Cooper and Cooper, 2008; Munro and Munro, 2008). The entry of the bullet or pellet into the myocardial layer or pericardial space can result in hemopericardium and cardiac tamponade, conditions that hamper ventricular filling and can eventually lead to cardiogenic shock (Elliott and Mayhew, 2011). The rising pressure generated by the fluid buildup in the pericardial sac impedes diastolic filling and results in a profound drop in cardiac output (Pavletic and Trout, 2006; Munro and Munro, 2008). Acute tamponade is associated with an early mortality. In dogs, acute cardiac tamponade has been reported to develop within minutes following penetrating thoracic trauma and is associated with acute cardiac compression (Spodick, 1967). Because the pericardium is a relatively inelastic serofibrous sac, sudden increases in intrapericardial fluid volume cannot be rapidly accommodated. Consequently, diastolic filling is restricted, leading to a reduction in venous return and stroke volume, ultimately resulting in circulatory collapse and cardiogenic shock (Tilley et al., 2024). Cardiac tamponade begins when the normally negative pericardial pressure equilibrates with the right atrium and ventricle diastolic pressures. When intrapericardial pressure rises to positive values typically exceeding 12 cm H2O, the right atrial and/or right ventricular free wall collapses, with a consequent decline in cardiac output. This process may lead to cardiogenic shock and sudden death in acute cases, whereas chronic fluid accumulation may result in right-sided heart failure (Shaw and Rush, 2007; Boon, 2011). In this case, approximately 100–150 ml of clotted blood was detected within the pericardial cavity. Previous studies have indicated that even relatively small but rapidly accumulating volumes of blood (200–400 ml) can cause fatal pericardial compression and circulatory failure in acute hemopericardium (Shaw and Rush, 2007; Boon, 2011). Although direct penetrating cardiac injury was present, the synchronous impact of multiple shotgun pellets to the thorax, causing sudden intrathoracic pressure transmission and energy transfer, may have been one of the primary causes of death in this case. In this case, approximately 100–150 ml of clotted blood was detected within the pericardial cavity. Although the exact volume could not be quantified, this amount was sufficient to suggest acute cardiac tamponade, consistent with previous studies reporting that even 200–400 ml of rapidly accumulating blood can cause fatal circulatory collapse in dogs (Shaw and Rush, 2007; Boon, 2011). The jugular vein exhibited perivascular hemorrhage and partial mural disruption rather than complete rupture, indicating limited external bleeding that may have contributed to systemic blood loss. Together with evidence of myocardial penetration and pericardial coagulum, these findings support a multifactorial mechanism of death primarily involving cardiac tamponade and myocardial injury, with possible additive effects of vascular hemorrhage from the cervical region (Kneubuehl et al., 2011; Le Garff et al., 2015; Piegari et al., 2024). Concurrent pulmonary hemorrhage and emphysematous changes observed histologically are consistent with secondary barotrauma and internal pressure fluctuations following multiple high-energy impacts, in agreement with previous descriptions of ballistic lung trauma in dogs (Alcigir et al., 2014). Based on the radiographic, gross, and histopathological findings, the injuries appear to have resulted from multiple rapid discharges. The lesions in the cervical region, particularly around the jugular vein and directed toward the heart, indicate that the first shot was the most likely lethal event (Cooper and Cooper, 2008; Kneubuehl et al., 2011; Le Garff et al., 2015). The absence of thermal damage, hemorrhagic halo, or gunpowder residue in other anatomical areas indicates that these lesions developed postmortem or secondary to pellet displacement. Altogether, the observations support the interpretation that the shots were fired from a long range and sequentially, and that jugular vein rupture, cardiac tamponade, and hemothorax represent the primary lethal consequences of the initial discharge directed toward the cervical and thoracic regions (Felsmann et al., 2012). When animals suffer gunshot injuries, both the direct effects of traumatic penetration and the tissue and systemic changes caused by shock waves are considered vital (Cooper and Cooper, 2008). In the present case, the finding of hemorrhage in the bronchi, bronchioles, and alveoli, with emphysematous changes, indicates internal pressure changes and pulmonary hemorrhage. These findings are consistent with the macroscopic changes described by Alcigir et al. (2014) in a dog with ballistic lung trauma. In veterinary forensic pathology, perilesional hemorrhage, pellet tracks, coagulation necrosis, and particulate residues at the point of wound entry are very significant in evaluating firearm injuries. Histopathological and macroscopic characteristics have been observed during forensic necropsy in animals that had died due to gunshot (Piegari et al., 2024). Extensive soot particles on the surface of the tissue, abrasion rings, and extensive hemorrhage and necrosis in subcutaneous tissues are mentioned in contact shots, whereas these characteristics tend to diminish in distant-range shots, and tissue responses are limited. Microscopically, extensive areas of hemorrhage with yellowish granular material and inflammatory responses have been noted along the trajectory of the projectile. Piegari et al. (2024) discovered this particulate material to be residual Pb particles. In the current instance, yellowish granular material and hemorrhagic foci were observed in the lungs, heart, kidneys, and small intestine submucosa, supporting the results reported by Piegari et al. (2024). The intensity of the kinetic energy is the primary indicator of the severity of tissue damage caused by a projectile. Kneubuehl et al. (2011) and Ordog et al. (1984) reported that 5–15 J kinetic energy may cause skin penetration and subcutaneous tissue injury, 15–30 J may cause muscular injury, and energies >30 J may cause bone fracture and fatal internal organ injury (Table 3). In this case, the pellets were estimated to contain approximately 13-J kinetic energy sufficient to cause penetrating trauma in superficial tissues, such as the scalp. In fact, several perforating wounds were observed on the scalp. Nevertheless, the absence of skull penetration and damage or the presence of residual material within the brain suggests that this much energy was insufficient to penetrate the cranial bone barrier. Table 3. Potential tissue effects based on kinetic energy levels (in Joules).
ConclusionIn conclusion, limiting ballistic analysis, macroscopic, and histopathological analysis provided significant guidance to the determination of the nature of trauma and cause of death—that is, injury of multiple organs resulting in hypovolemic and cardiogenic shock—even though the firearm used in this incident was not confiscated. Thus, the case is a classic illustration of the utility of necropsy analysis in veterinary forensic pathology. AcknowledgmentsThe authors declare that there are no individuals or institutions to acknowledge. Conflict of interestThe authors declare no conflict of interest. FundingNone. Authors’ contributionsLatife Çakır Bayram: Design and conduct of the study, review, and approval of the final version of the article. Gültekin Atalan: Clinical examination and evaluation of radiographic images. Gökçen Perk: Clinical examination, radiographic evaluation, and reporting. Görkem Ekebaş: Conducting necropsy and laboratory procedures and writing the article. Kübra Yağlı: Necropsy, laboratory procedures, and writing the article. Ethical approvalEthical approval was not required for this study because the case represented a forensic necropsy conducted under judicial authorization. The animal was submitted for postmortem examination following an official request from the Office of the Public Prosecutor, and all procedures were performed in accordance with national forensic and veterinary regulations. Data availabilityAll data were provided in the manuscript. ReferencesAksoy, E., Çoltu, A., Ege, B., Günaydın, G, Inanıcı MA, Karali H, Karagöz M, Ötker C, Yemisçigil A. 2013. Adli Travmatoloji. Available via http://www.ttb.org.tr/eweb/adli/4.html (Accessed 15 Jan 2013). Alcigir, M.E., Vural, S.A. and Alcigir, G. 2014. Evaluation of patho-morphological changes associated with a firearm injury in terms of wound ballistic in a dog. Res. J. Vet. Pract. 2(5), 78–81. Barach, E., Tomlanovich, M. and Nowak, R. 1986. Ballistics: a pathophysiologic examination of the wounding mechanisms of firearms. J. Trauma 26, 225–235. Boon, J.A. 2011. Manual of Veterinary Echocardiography. 2nd ed., Baltimore, MD: Williams & Wilkins. Bradley-Siemens, N. and Brower, A.I. 2016. Veterinary Forensics: firearms and Investigation of Projectile Injury. Vet. Pathol. 53(5), 988–1000; doi:10.1177/0300985816653170 Capak, H., Capak, D., Simpraga, M., Kos, J. and Mikus, T. 2016. Radiographic findings in dogs with firearm injuries: a retrospective study of 166 cases (2010–2014). Vet. Arhiv. 86(1), 1–15. Cooper, G.J. and Ryan, J.M. 1990. Interaction of penetrating missiles with tissues. Br. J. Surg. 77, 606–610. Cooper, J.E. and Cooper, M.E. 2008. Forensic veterinary medicine: a rapidly evolving discipline. Forensic Sci. Med. Pathol. 4, 75–82. Crofts, S.L., Rousset, E., Day, J. and Sharp, C.R. 2023. Increased incidence and shift in the location of gunshot wound injuries in companion animals: a 10-year review. J. Am. Vet. Med. Assoc. 261(12), 1495–1503; doi:10.2460/javma.23.06.0317 DeCook, J.R., Rochat, M.C., Payton, M.E. and Cantwell, H.D. 2001. Gunshot injuries in dogs and cats: 37 cases (2001–2010). J. Am. Vet. Med. Assoc. 245(8), 923–928; doi:10.2460/javma.245.8.923 Elliott, J.M. and Mayhew, P.D. 2011. Diagnostic challenges and treatment options of a suspected pericardial metallic projectile foreign body in a dog. J. Vet. Emerg. Crit. Care. (San. Antonio). 21(6), 684–691. Felsmann, M.Z., Szarek, J., Felsmann, M. and Babińska, I. 2012. Factors affecting temporary cavity generation during gunshot wound formation in animals – new aspects in the light of flow mechanics: a review. Medycyna Weterynaryjna 68(10), 600–604. Fox, P.R., Hohenhaus, A.E. and Kharbush, R.J. 2020. Air Gun Ballistic Projectile Lodged in the Interventricular Septum of an Asymptomatic Dog. CASE (Phila). 30(6), 531–533. Grela, M., Panasiuk-Flak, K., Listos, P., Gryzińska, M., Buszewicz, G., Chagowski, W. and Teresiński, G. 2021. Post-mortem analysis of gunshot wounds to the head and thorax in dogs by computed tomography, radiography and forensic necropsy. Med. Sci. Law 61, 105–113. Khankhasykov, S.P., Zhilin, D.N. and Tokar VV. Gunshot wounds to animals. BIO Web Conf. 2024;108:03011. doi: 10.1051/bioconf/202410803011. Kneubuehl, B.P., Coupland, R.M., Rothschild, M.A. and Thali, M.J. 2011. Wound Ballistics: basics and Applications. Berlin, Germany: Springer. Le Garff, E., Delannoy, Y., Mesli, V., Berthezene, J.M., Morbidelli, P. and Hédouin, V. 2015. Homemade firearm suicide with dumbbell pipe triggering by an air-compressed gun: case report and review of literature. Am. J. Forensic Med. Pathol. 36, 257–261. Munro, R. and Munro, H.M.C. 2008. Firearms injuries.In Animal Abuse and Unlawful Killing: forensic Veterinary Pathology. Munro R Munro., HMC. and eds. Saunders Edinburgh, UK: Elsevier, pp: 55–64. Olsen, L.E., Streeter, E.M. and DeCook, R.R. 2014. Review of gunshot injuries in cats and dogs and utility of a triage scoring system to predict short-term outcome: 37 cases (2003–2008). J. Am. Vet. Med. Assoc. 245(8), 923–929; doi:10.2460/javma.245.8.923. Ordog, G.J., Wasserberger, J. and Balasubramanium, S. 1984. Wound ballistics: theory and practice. Ann. Emerg. Med. 13(12), 1113–1122; doi:10.1016/s0196-0644(84)80336-4 Pavletic, M.M. and Trout, N.J. 2006. Bullet, bite, and burn wounds in dogs and cats. Vet. Clin. North. Am. Small. Anim. Pract. 36, 873–893. Piegari, G., d’Aquino, I., Salanti, G.V., Romano, V., Miletti, G., Sannino, E., Di Napoli, E., Riccio, L., De Biase, D. and Paciello, O. 2024. Pathological Changes and Sodium Rhodizonate Test as Tools for Investigating Gunshot Wounds in Veterinary Forensic Pathology. Animals (Basel). 9(19), 2913. Shaw, D.H. and Rush, J.E. 2007. Canine and feline cardiology. St. Louis, MO: Saunders Elsevier. Spodick, D.H. 1967. Acute cardiac tamponade pathologic physiology, diagnosis and management. Prog. Cardiovasc. Dis. 10(1), 64–96; doi:10.1016/s0033-0620(67)80006-9 Tilley, L.P., Smith, F.W. and Sleeper, M.M. 2024. Manual of Canine and Feline Cardiology-E-BOOK. St. Louis, MO: Elsevier Health Sciences. | ||



| How to Cite this Article |
| Pubmed Style Yağlı K, Ekebaş G, Perk G, Atalan G, Bayram LC. Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. Open Vet. J.. 2026; 16(1): 731-738. doi:10.5455/OVJ.2026.v16.i1.69 Web Style Yağlı K, Ekebaş G, Perk G, Atalan G, Bayram LC. Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. https://www.openveterinaryjournal.com/?mno=276008 [Access: June 26, 2026]. doi:10.5455/OVJ.2026.v16.i1.69 AMA (American Medical Association) Style Yağlı K, Ekebaş G, Perk G, Atalan G, Bayram LC. Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. Open Vet. J.. 2026; 16(1): 731-738. doi:10.5455/OVJ.2026.v16.i1.69 Vancouver/ICMJE Style Yağlı K, Ekebaş G, Perk G, Atalan G, Bayram LC. Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. Open Vet. J.. (2026), [cited June 26, 2026]; 16(1): 731-738. doi:10.5455/OVJ.2026.v16.i1.69 Harvard Style Yağlı, K., Ekebaş, . G., Perk, . G., Atalan, . G. & Bayram, . L. C. (2026) Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. Open Vet. J., 16 (1), 731-738. doi:10.5455/OVJ.2026.v16.i1.69 Turabian Style Yağlı, Kubra, Gorkem Ekebaş, Gokcen Perk, Gultekin Atalan, and Latife Cakır Bayram. 2026. Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. Open Veterinary Journal, 16 (1), 731-738. doi:10.5455/OVJ.2026.v16.i1.69 Chicago Style Yağlı, Kubra, Gorkem Ekebaş, Gokcen Perk, Gultekin Atalan, and Latife Cakır Bayram. "Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings." Open Veterinary Journal 16 (2026), 731-738. doi:10.5455/OVJ.2026.v16.i1.69 MLA (The Modern Language Association) Style Yağlı, Kubra, Gorkem Ekebaş, Gokcen Perk, Gultekin Atalan, and Latife Cakır Bayram. "Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings." Open Veterinary Journal 16.1 (2026), 731-738. Print. doi:10.5455/OVJ.2026.v16.i1.69 APA (American Psychological Association) Style Yağlı, K., Ekebaş, . G., Perk, . G., Atalan, . G. & Bayram, . L. C. (2026) Forensic evaluation of a fatal shotgun injury in a Cane Corso dog: Necropsy and radiographic findings. Open Veterinary Journal, 16 (1), 731-738. doi:10.5455/OVJ.2026.v16.i1.69 |

