




| Original Article | ||
Open Vet J. 2022; 12(6): 975-979 Open Veterinary Journal, (2022), Vol. 12(6): 975–979 Original Research Comparison of osteotomy level with three different canine total hip replacement systemsSamuel P. Franklin1,2,3*, Ashley L. Franklin1,2, Nathan Feyerabend2, Kei Hayashi4, Nathan A. Miller3 and James L. Cook21Kansas City Canine Orthopedics, 21648 Midland Drive, Shawnee, Kansas 66218, USA 2Thompson Laboratory for Regenerative Orthopaedics, University of Missouri, Missouri Orthopaedic Institute, Columbia, MO 65212, USA 3Colorado Canine Orthopedics, 55218 N. Nevada Avenue, Colorado Springs, CO 80918, USA 4JD Wheat Veterinary Orthopedic Research Laboratory, School of Veterinary Medicine, University of California Davis, Davis, CA 95616, USA Submitted: 03/08/2022 Accepted: 13/11/2022 Published: 13/12/2022 *Corresponding Author: Samuel P. Franklin, Kansas City Canine Orthopedics, Shawnee, KS. Email: samfranklin [at] kck9ortho.com © 2022 Open Veterinary Journal
AbstractBackground: Numerous cementless total hip replacement (THR) systems are available for application in dogs and one of the potential differences among these systems is the technique for performing a femoral osteotomy and the amount of bone preserved in the calcar region. However, no quantitative comparison of osteotomy level has been performed for canine THRs to date. Aims: To develop and validate a method for quantifying the level of the osteotomy at its most distomedial aspect in conjunction with canine THR and to compare osteotomy level between multiple different THRs. Methods: Immediate post-operative cranial-caudal or caudal-cranial radiographs of 33 dogs treated with 17 Helica and 17 BFX THR were assessed and osteotomy level was quantified using a novel radiographic assessment by 3 independent observers. Correlation among observers was quantified using a Spearman rank order correlation. Osteotomy location was subsequently quantified for an additional 10 Zurich THRs. The osteotomy level for each THR was subsequently compared between Helica, BFX, and Zurich THRs using one-way non-parametric Mann–Whitney rank sum tests and significance set at p < 0.05. Results: R-values assessing correlation between observers were 0.87, 0.72, and 0.60. Osteotomy location was significantly more proximal in conjunction with the Helica (0.75 ± 0.22) versus the BFX (0.97 ± 0.13; p < 0.001) and Zurich (1.1 ± 0.15; p < 0.001) femoral prostheses. Osteotomy location was also significantly more proximal with the BFX prosthesis in comparison to the Zurich THR (p < 0.05). Conclusion: The strong correlations among three different observers indicate that the technique for measuring the location of the distomedial aspect of the osteotomy was acceptably precise. The osteotomies made in conjunction with the short-stemmed Helica implants were significantly more proximal than those made with both of the long-stemmed (BFX and Zurich) femoral prostheses. The distomedial aspect of the osteotomy with the BFX system was significantly more proximal than that with the Zurich THR, indicating that between these two long-stemmed systems the osteotomy level is unique. Keywords: Canine, Osteotomy, Total hip replacement. IntroductionNumerous cementless total hip replacement (THR) systems are now available for use in canine patients including long-stemmed prostheses such as the BFX (Biomedtrix, Boonton, NJ) and Zurich (KYON, Zurich, Switzerland) systems, as well as short-stemmed prostheses such as the Helica (Innoplant, Hannover, Germany) and Centerline (Biomedtrix, Boonton, NJ) implants. Each of these systems likely has advantages and disadvantages associated with the prosthesis design and technique for implantation. Understanding the nuances of each system could highlight pros and cons of each, help surgeons choose among systems (either for an individual patient or as a whole), and assist with surgical execution. One aspect of canine THRs that have not been quantitatively compared among systems is the level of the distomedial aspect of the osteotomy in the calcar region. This aspect of THR is clinically relevant because bone stock in the calcar region can limit stability of an implanted femoral prosthesis. Accordingly, implants that preserve more proximal femoral bone stock might be advantageous if revision of the implant were ever needed. Conversely, if revision of a failed previous THR or a femoral head and neck ostectomy is being performed, a THR system that typically has the lowest femoral osteotomy and requires the least amount of bone in the calcar region might be an optimal revision choice. In addition to relevance to revision surgery, understanding the appropriate location of the osteotomy can affect implant placement during an index THR and in turn, affect outcomes. It was previously found that transitioning from the BFX system to the Zurich system was accompanied by the first author performing osteotomies that were higher than ideal for the Zurich system (Franklin et al., 2021). Accordingly, a high proportion of these dogs were implanted with a short neck prosthesis, which can decrease hip range of motion (Franklin et al., 2021). While predilection for performing a proximal BFX-style osteotomy was proposed as a potential explanation for why a great number of short or extra short femoral necks were needed in those patients, there has been no quantitative comparison of osteotomy level among different THR systems to our knowledge. The first objective of this study was to develop and test precision of a method for characterizing the location of the osteotomy at its most distomedial aspect. The second objective was to compare the osteotomy level (distomedial aspect specifically) of three different THR systems (Helica, BFX, and Zurich). We hypothesized that our methodology for assessing femoral osteotomy location would be adequately repeatable among three different observers for application. We also hypothesized that the osteotomy with the short-stemmed, neck-preserving Helica system would be significantly more proximal than that with the BFX and Zurich long-stemmed prostheses. In addition, based on our previous experience with BFX and Kyon THRs and previous publication (Franklin et al., 2021), we hypothesized that the osteotomy with the BFX system would be significantly more proximal than that with the Zurich system. Materials and MethodsImmediate post-operative cranial-caudal or caudal-cranial radiographs of 34 femurs from 33 patients were evaluated to assess the level of the osteotomy used with 17 Helica and 17 BFX femoral prostheses. Fourteen of the Helica prostheses were placed at University of California-Davis in 13 patients and 3 were implanted in 3 patients at the University of Missouri and included all THR with the Helica system at these 2 locations at the time of this study. Seventeen patients with a BFX femoral prosthesis at the University of Missouri were sequentially selected from those THR performed at this institution during the same time frame as the performance of the Helica THRs in order to provide a comparative cohort. Cases were included if radiographic positioning was considered appropriate for assessment of the femoral osteotomy. Radiographic positioning was considered appropriate if the patella was centered in the trochlear groove, the fabella was bisected by the distal femoral cortices, and a portion of the lesser trochanter was visible on the cranial-caudal view. Furthermore, radiographs were considered unacceptable if there was radiographically obvious foreshortening of the femur, that would result from the femur not being perpendicular to the radiographic beam. The level of the osteotomy was evaluated by first creating a vertical reference line (VRL) that was defined distally by the most distal medial aspect of the intertrochanteric fossa (point C; Fig. 1). The proximal end of the line was defined by making the line tangential to the medial aspect of the greater trochanter. Three points were then identified on the proximal femur. The most proximal aspect of the greater trochanter was identified (point A) and a line perpendicular to the VRL was drawn through this point and accordingly named line A. Next, the most distomedial aspect of the femoral osteotomy was identified (point B). A line perpendicular to the VRL was established through this location and was named line B. Lastly, a line perpendicular to the VRL was established through the most distal medial aspect of the intertrochanteric fossa (i.e., point C), and was named line C. The distances between lines A and B and A and C were measured and the ratio of the length AB to AC was calculated (AB/AC ratio; effectively the ratio of the distance from the greater trochanter to the femoral osteotomy relative to the distance between the greater trochanter and the distal aspect of the intertrochanteric fossa). Larger ratios were consistent with a more distal osteotomy and small ratios were indicative of a more proximal osteotomy. All measurements were made by three observers of differing levels of experience working independently. The observers were the primary author (SPF; observer 1), a general practice veterinarian (ALF; observer 2), and a veterinary student (NF; observer 3). Inter-observer correlation was assessed using a Spearman rank order correlation. Subsequent to assessment of precision, the ratio AB/AC was measured by the primary author (SPF) for 10 Zurich THRs on immediate post-operative cranial-caudal or yoga-style radiographs. Cases were included if radiographic positioning enabled the identification of the aforementioned landmarks. These were Zurich THRs performed as part of another study, and for which radiographs were available for review and measurement (Franklin et al., 2021). The ratio of AB/AC as measured by the primary author was compared between the Helica and BFX systems, the Helica and Zurich systems, and the BFX and Zurich systems using non-parametric Mann–Whitney rank sum tests. Given the hypotheses made a priori were one-sided, significance was set at a p-value of 0.05 for one-sided tests.
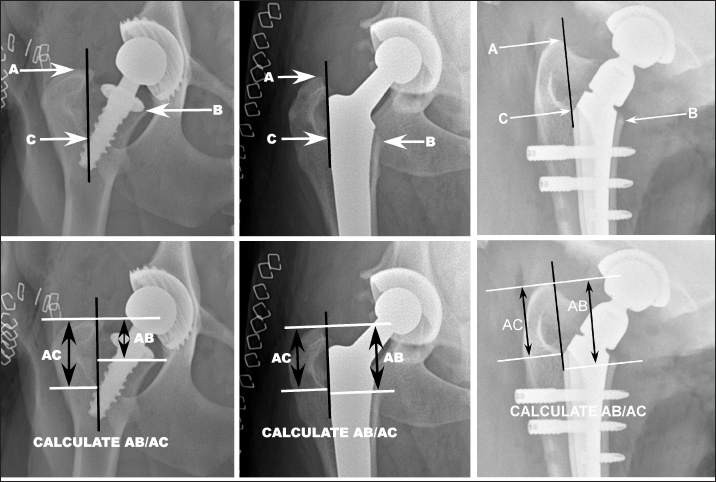
Fig. 1. A VRL (black) was defined distally by the most distal medial aspect of the intertrochanteric fossa (point C). The proximal end of the line was defined by making the line tangential to the medial aspect of the greater trochanter. Three points were then identified on the proximal femur. The most proximal aspect of the greater trochanter was identified (point A) and a line perpendicular to the VRL was drawn through this point and accordingly named line A. Next, the most distal-medial aspect of the femoral osteotomy was identified (point B). A line perpendicular to the VRL was established through this location and was named line B. Lastly, a line perpendicular to the VRL was established through the aforementioned point C, the most distal medial aspect of the intertrochanteric fossa, and was named line C. The distances between lines A and B and A and C were measured and the ratio of the length AB to AC was calculated (AB/AC ratio). Larger ratios were considered consistent with a more distal osteotomy and small ratios were considered indicative of a more proximal osteotomy. Representative images of Helica (far left), BFX (middle), and Zurich (right) THRs are included. This was a radiograph review study of client-owned dogs that underwent a THR. All owners provided written consent for surgical treatment (THR) of their dog. ResultsThe r-value assessing the correlation between observers 1 and 2 was 0.72. The r-value assessing correction between observers 1 and 3 was 0.87, and the r-value assessing correction between observers 2 and 3 was 0.60. The mean AB/AC ratio for the femurs implanted with a Helica prosthesis was 0.75 (±st. dev. 0.22), 0.97 (±0.13) for the femurs implanted with a BFX femoral component, and 1.1 (±0.15) for the Zurich system (smaller ratios are indicative of a more proximal osteotomy). Based on the Mann–Whitney rank sum test, the difference between the Helica and BFX systems was statistically significant ( p=0.00009). The difference between the Helica and Zurich system was statistically significant ( p=0.00024). Lastly, the difference between the BFX and Zurich systems was statistically significant (p=0.025) with the BFX having a more proximal osteotomy. DiscussionThe first objective of this study was to develop and validate a method for quantifying the level of the osteotomy at its most distomedial aspect in conjunction with canine THR. The landmarks used were based in part on landmarks previously described for assessing the BFX femoral prosthesis (Lascelles et al., 2010). Those investigators used a VRL in the cranial-caudal view that was placed along the lateral aspect of the BFX stem and which was very similar to the VRL along the medial aspect of the intertrochanteric fossa in this study (Lascelles et al., 2010). In addition, those investigators used the most distal medial aspect of the intertrochanteric fossa immediately adjacent to the BFX stem as a reference point for assessing subsidence of the BFX implant (Lascelles et al., 2010). We used that same point (point C) in this study. The other landmarks that we chose for this study were selected based upon their ease of identification and their clinical relevance. The proximal aspect of the greater trochanter is readily identifiable and therefore was considered a good choice for one reference location. Similarly, the distomedial aspect of the osteotomy is radiographically apparent and is clinically relevant as presence of sufficient bone in the calcar region may affect feasibility of THR revision. The results from this study indicate that the landmarks we used could be reproducibly identified by different observers, even when including observers with little veterinary surgical experience. This conclusion is supported by the strong to very strong correlations. As a result, we accepted our first hypothesis and concluded that the landmarks used were radiographically identifiable and the methodology developed was adequately precise. The second objective of this study was to compare the level of the distomedial aspect of the osteotomy among three different THR systems. The data showed that the osteotomy was significantly higher with the short-stemmed Helica system than with both of the long-stemmed prostheses (BFX and Zurich). This result is plausible, if not intuitive, given that with the Helica system the surgeon removes the femoral head and places the prosthesis within the femoral neck, rather than placing the implant into the femoral diaphysis. However, confirmation, rather than assumption, that bone stock is preserved at the distomedial aspect of the osteotomy with the Helica THR is relevant because this could facilitate revision to a long-stemmed prosthesis if a complication were to occur. Indeed, in human medicine, one of the motivations for use of neck-preserving hip resurfacing prostheses in young patients is the preservation of bone stock and ability to revise to a long-stemmed prosthesis when the index implant wears (Clough and Clough, 2021). Although this may be a less common consideration in canine medicine, it is relevant as an increasing number of reports describe performing THR in juvenile dogs, coupled with reports of canine THR implant wear, breakage, or need for revision (Guerrero and Montavon, 2009; Fitzpatrick et al., 2014; Vezzoni et al., 2015; Ficklin et al., 2016; Nesser et al., 2016; DiVincenzo et al., 2017; Vezzoni et al., 2017). These publications indicate that preservation of bone stock and the ability to revise the THR is clinically relevant for some dogs. The data also indicated that the osteotomy performed with the BFX THR was significantly more proximal than that made with the Zurich THR. This comparison was motivated in part by a previous study in which the first author transitioned from the BFX to the Zurich system and recognized that (subjectively) reduction of the Zurich femoral implant was consistently challenging, that the neck prostheses applied in that study were shorter than ideal, and the speculation that the osteotomy with the Zurich THR should be made more distally than with the BFX system (Franklin et al., 2021). Hence, we sought to test the hypothesis that the osteotomy level is more proximal with the BFX system and the data support this hypothesis. This finding is clinically relevant for two reasons. First, for those surgeons using both systems or transitioning between systems, recognition of the need for performing a system-specific osteotomy is needed to help facilitate the use of optimal femoral neck lengths with the Zurich system and facilitate manageable reduction of the femoral component. Second, the Zurich femoral implant may be the optimal choice for revision of a failed index THR, or femoral head and neck excision, where bone stock in the calcar region is limited. This latter presumption is supported in part by a report of revision of two cases of BFX THR to Zurich THR (Vezzoni et al., 2017). There are a few limitations of this study. In terms of radiographic positioning, we used landmarks and positioning of the femur to make sure there was not internal or external rotation of the femur. However, we cannot be assured that the radiographic beam was exactly 100% perpendicular to the frontal plane of the femur. This would require that simultaneous radiographic or fluoroscopic imaging be made in the sagittal plane. Performing bi-planar radiography has not been the standard in studies assessing femoral implant positioning and we suspect that positioning was adequate in this study to support the data and conclusions made. In addition, there can be variability in the height or distance between the proximal aspect of the greater trochanter and the base of the intertrochanteric fossa, which could have affected results. We think that it is unlikely that results were substantially changed by inter-individual variability because this measurement was not an absolute measurement, but rather was the denominator of a ratio to determine the relative proximity of the osteotomy. For these factors, radiographic positioning and methodology of osteotomy level, we used landmarks and positioning that have been used commonly in prior studies, were repeatable among observers in this study with strong inter-observer correlations, and provided plausible results. An additional limitation that should be mentioned is that, the osteotomy level is ultimately controlled by each individual surgeon and so these results apply to the authors and may not be representative of osteotomies performed by all surgeons. However, all the surgeons in this study were experienced, performed the THRs according to the accepted techniques for each system, and the results of this study are plausible based upon nstructions for how to perform the associated femoral osteotomy with each of these different THRs. As a result, we believe the results of this study are likely widely applicable. Most importantly, it is relevant to highlight that this study is not a comprehensive comparison of different THR systems and is not meant to suggest that one system is superior to another. Rather, osteotomy level is just one of many attributes that could be considered when selecting a THR femoral implant for a particular patient. AcknowledgmentsWe thank Howard Wilson and Donald Connor for their assistance with figure preparation. We thank Richard Hurt for facilitating study completion. Conflict of interestDr. Franklin and Dr. Miller have taught THR courses using the Zurich THR system but have no royalties or financial incentive in this system. Authors’ contributionsS.P.F. conceived the study, collected and analyzed data, and drafted the manuscript. A.L.F. and N.F. performed data collection/measurements. K.H., N.M., and J.L.C. all performed or assisted with the performance of the THRs. All authors provided conceptual input on the study design and data collection and reviewed and approved the manuscript. ReferencesClough, E.J. and Clough, T.M. 2021. Metal on metal hip resurfacing arthroplasty: where are we now? J. Orthop. 23, 123–127. DiVincenzo, M.J., Frydman, G.H., Kowaleski, M.P., Vanderburg, C.R., Lai, B., Oura, T.J. and Jennings, S.H. 2017. Metallosis in a dog as a long-term complication following total hip arthroplasty. Vet. Pathol. 54, 828–831. Ficklin, M.G., Kowaleski, M.P., Kunkel, K.A. and Suber, J.T. 2016. One-stage revision of an infected cementless total hip replacement. Vet. Comp. Orthop. Traumatol. 29, 541–546. Fitzpatrick, N., Law, A.Y., Bielecki, M. and Girling, S. 2014. Cementless total hip replacement in 20 juveniles using BFX™ arthroplasty. Vet. Surg. 43, 715–725. Franklin, S.P., Miller, N.A. and Riecks, T. 2021. Complications with the Zurich canine total hip replacement system in an initial series of cases performed by a single surgeon. Vet. Comp. Orthop. Traumatol. 34, 346–351. Guerrero, T.G. and Montavon, P.M. 2009. Zurich cementless total hip replacement: retrospective evaluation of 2nd generation implants in 60 dogs. Vet. Surg. 38, 70–80. Lascelles, B.D.X., Freire, M., Roe, S.C., Depuy, V., Smith, E. and Marcellin-Little, D.J. 2010. Evaluation of functional outcome after BFX total hip replacement using a pressure sensitive walkway. Vet. Surg. 39, 71–77. Nesser, V.E., Kowaleski, M.P. and Boudrieau, R.J. 2016. Severe polyethylene wear requiring revision total hip arthroplasty in three dogs. Vet. Surg. 45, 664–671. Vezzoni, L., Bazzo, S. and Vezzoni, A. 2017. Revision of a BFX total hip replacement stem using a Kyon stem and a head adaptor in two dogs. Vet. Comp. Orthop. Traumatol. 30, 81–87. Vezzoni, L., Vezzoni, A. and Boudrieau, R.J. 2015. Long-term outcome of Zürich cementless total hip arthroplasty in 439 cases. Vet. Surg. 44, 921–929. | ||
| How to Cite this Article |
| Pubmed Style Franklin S, Franklin A, Feyerabend N, Hayashi K, Miller N, Cook JL. Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. Open Vet J. 2022; 12(6): 975-979. doi:10.5455/OVJ.2022.v12.i6.25 Web Style Franklin S, Franklin A, Feyerabend N, Hayashi K, Miller N, Cook JL. Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. https://www.openveterinaryjournal.com/?mno=90414 [Access: July 01, 2025]. doi:10.5455/OVJ.2022.v12.i6.25 AMA (American Medical Association) Style Franklin S, Franklin A, Feyerabend N, Hayashi K, Miller N, Cook JL. Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. Open Vet J. 2022; 12(6): 975-979. doi:10.5455/OVJ.2022.v12.i6.25 Vancouver/ICMJE Style Franklin S, Franklin A, Feyerabend N, Hayashi K, Miller N, Cook JL. Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. Open Vet J. (2022), [cited July 01, 2025]; 12(6): 975-979. doi:10.5455/OVJ.2022.v12.i6.25 Harvard Style Franklin, S., Franklin, . A., Feyerabend, . N., Hayashi, . K., Miller, . N. & Cook, . J. L. (2022) Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. Open Vet J, 12 (6), 975-979. doi:10.5455/OVJ.2022.v12.i6.25 Turabian Style Franklin, Samuel, Ashley Franklin, Nathan Feyerabend, Kei Hayashi, Nathan Miller, and James L. Cook. 2022. Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. Open Veterinary Journal, 12 (6), 975-979. doi:10.5455/OVJ.2022.v12.i6.25 Chicago Style Franklin, Samuel, Ashley Franklin, Nathan Feyerabend, Kei Hayashi, Nathan Miller, and James L. Cook. "Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems." Open Veterinary Journal 12 (2022), 975-979. doi:10.5455/OVJ.2022.v12.i6.25 MLA (The Modern Language Association) Style Franklin, Samuel, Ashley Franklin, Nathan Feyerabend, Kei Hayashi, Nathan Miller, and James L. Cook. "Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems." Open Veterinary Journal 12.6 (2022), 975-979. Print. doi:10.5455/OVJ.2022.v12.i6.25 APA (American Psychological Association) Style Franklin, S., Franklin, . A., Feyerabend, . N., Hayashi, . K., Miller, . N. & Cook, . J. L. (2022) Comparison of Osteotomy Level with Three Different Canine Total Hip Replacement Systems. Open Veterinary Journal, 12 (6), 975-979. doi:10.5455/OVJ.2022.v12.i6.25 |

